ESCR 2015 / P-0038
MRI of the Pericardium: What do we have to know? What do we have to look for?
Congress:
ESCR 2015
Poster Number:
P-0038
Type:
Scientific Poster
Keywords:
Anatomy, Cardiac, MR-Functional imaging, MR-Diffusion/Perfusion, Education, Cysts, Congenital, Pathology
Authors:
C. Saborido Avila, M. Rodríguez Álvarez, A. M. Afonso Centeno, B. Nieto Baltar, S. Barreiro Villalustre; VIGO/ES
DOI:
DOI-Link:
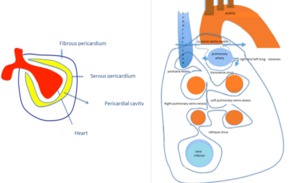
 The pericardium is formed by two layers, the fibrous outer layer and the inner serous layer, which folds on itself forming virtual pericardial cavity.
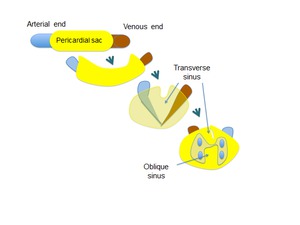
b)The transverse sinus is located behind the ascending aorta and pulmonary trunk and in front of the left atria and the superior vena cava.
The oblique sinus is an inverted U-shaped pericardial reflection located behind the left atrium.Pericardial recesses are sacculations of the pericardial cavity")
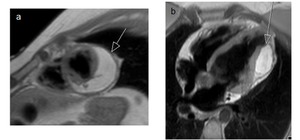
Fig. 1:
a) The pericardium is formed by two layers, the fibrous outer layer and the...

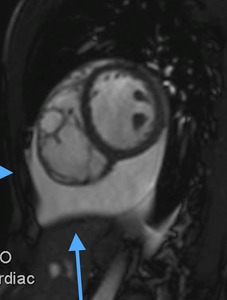
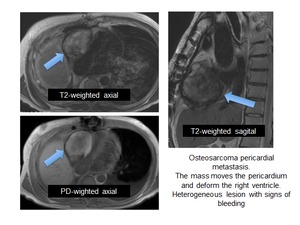
Fig. 2:
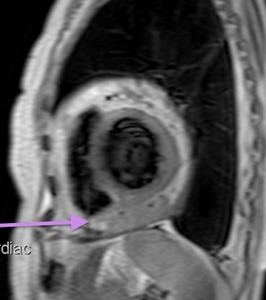
Cine MR Image, short axis. Peripheral severe pericardial effusion. Trasudate...

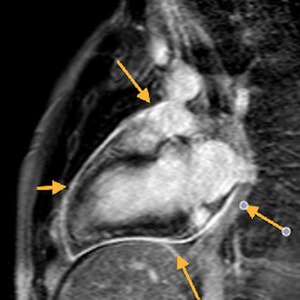
Fig. 3:
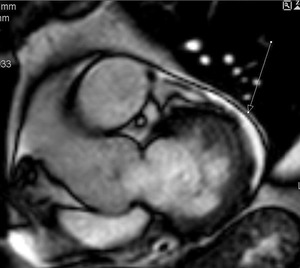
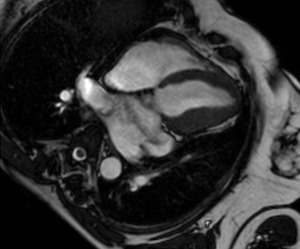
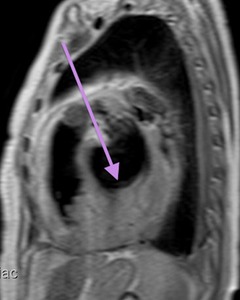
Long axis of the left ventricle, viability sequence, after IV gadolinium...

Fig. 4

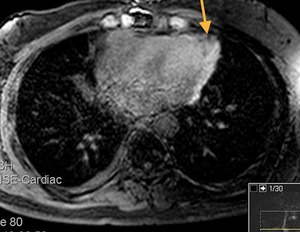
Fig. 5:
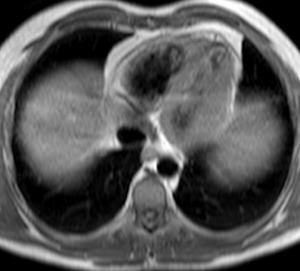
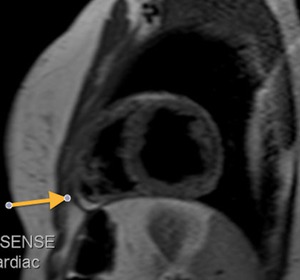
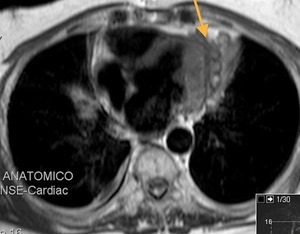
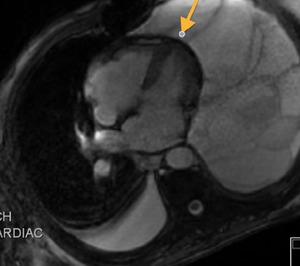
STIR, axial . The arrow shows the superior aortic recess

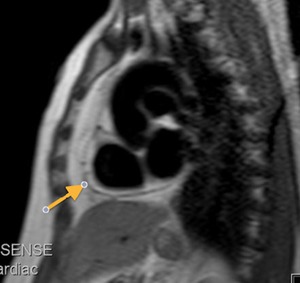
Fig. 6:
Black-blood T1-weighted image, axial. Patient with cystic lesion isointense to...

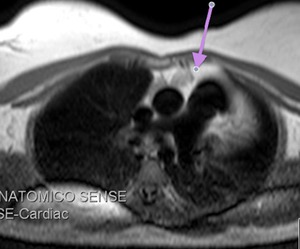
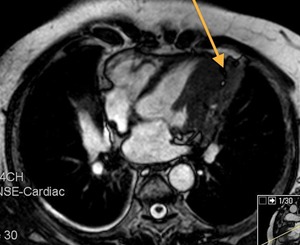
Fig. 7:
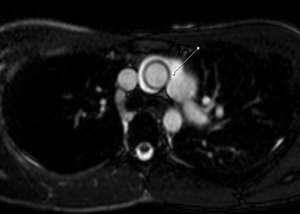
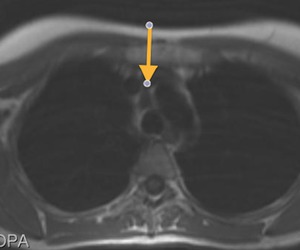
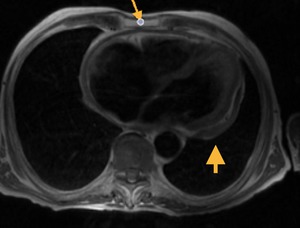
Superior aortic recess between the superior vena cava and the aorta. Axial...

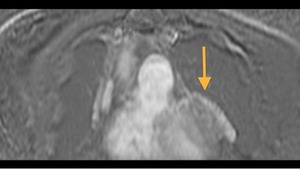
Fig. 8:
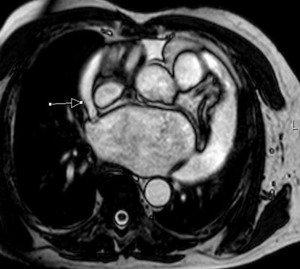
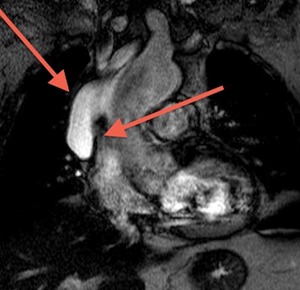
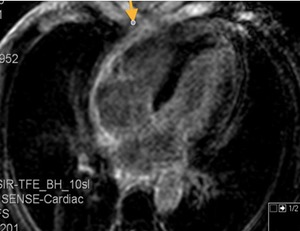
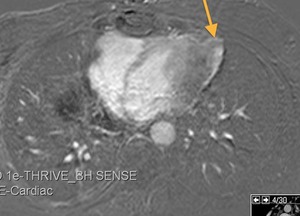
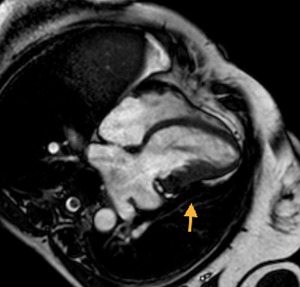
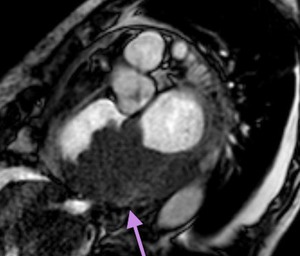
Cine MR Image. Patient with epicardial efussion. The arrow points to the right...

Fig. 9:
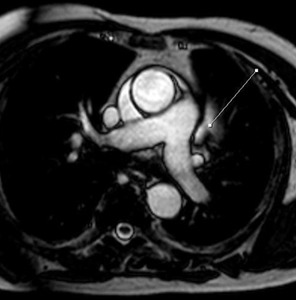
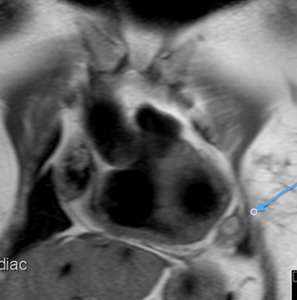
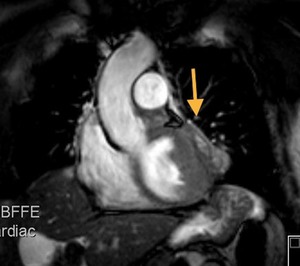
Cine MR image, axial. The arrow points to the left pulmonary artery recess.

Fig. 10:
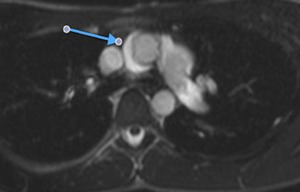
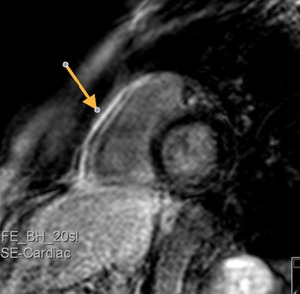
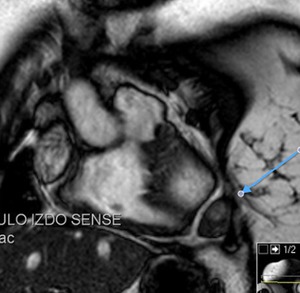
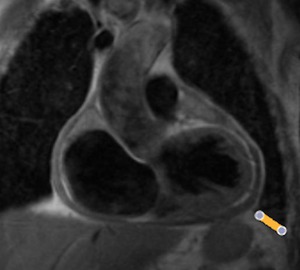
Cine MR image. Patient with pericardial effusion. The line shows the recess of...

Fig. 11:
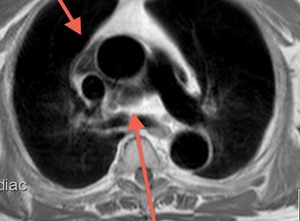
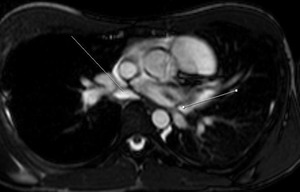
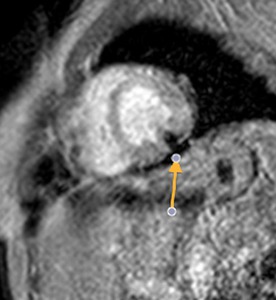
Cine MR image in a patient with pericardial effusion. The lines indicate the...

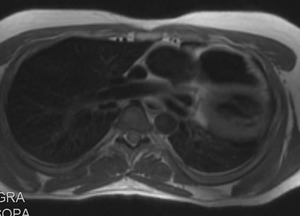
Fig. 12:
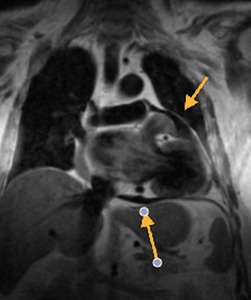
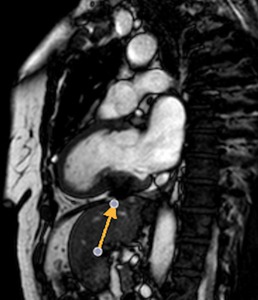
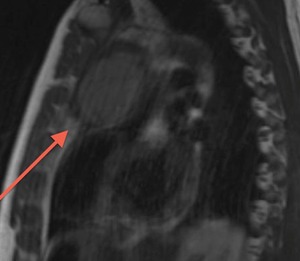
Black blood T1-weighted, coronal. Hypointense pericardial effusion in T1. The...

Fig. 13:
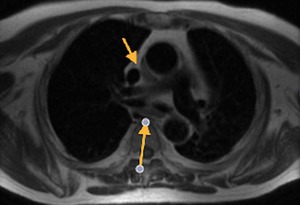
Black blood T1-weighted, axial. Anterior arrow points to the superior aortic...

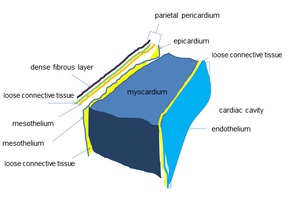
Fig. 14:
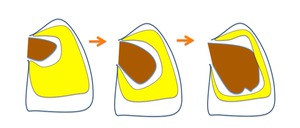
Development of the pericardial cavity. The heart develops invaginating the...

Fig. 15

Fig. 16:
Black-blood T1-weighted short axis image, shows severe peripheral effusion and...
, partially hyperintense on T1.")
Fig. 17:
Black-blood T1-weighted MR image,axial. Hematic pericardial effusion....
 image, axial. Hematic pericardial effusion, arrows, showing hypointense signal (the paramagnetic effect of hemosiderin)")
Fig. 18:
Gradient-echo (GE) image, axial. Hematic pericardial effusion, arrows, showing...

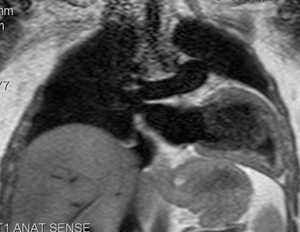
Fig. 19:
Black-blood T1-weighted MR image, sagittal. Complete agenesis of the left...

Fig. 20:
Black-blood T1-weighted MR image. Complete agenesis of the left pericardium ,...

Fig. 21:
T1-weighted, short axis. Patient with partial agenesis of the left pericardium....

Fig. 22:
Partial agenesis of the pericardium. Same patient as in the previous image....

Fig. 23:
T1-weighted image, coronal. Partial agenesis of the pericardium. The heart is...

Fig. 24:
Complete agenesis of the left pericardium.
Black-blood T1-weighted MR image,...

Fig. 26:
Partial agenesis of the pericardium.
Black-blood T1-weighted MR image, axial....

Fig. 25:
Partial agenesis of the pericardium. Black-blood T1-weighted MR image, axial....

Fig. 27:
Superior aortic recess between aorta and the superior cava.
T2-weighted MR...
.")
Fig. 28:
Fluid located in the superior aortic recess that persisted in the same location...

Fig. 29:
Liquid located in the superior aortic recess that persisted in the same...

Fig. 30:
Liquid located in the superior aortic recess that persisted in the same...

Fig. 31:
Liquid located in the superior aortic recess, with not diffusion restriction,...

Fig. 32:
Recurrent pericarditis. Black-blood T1-weighted MR image, axial.
Moderate...

Fig. 33:
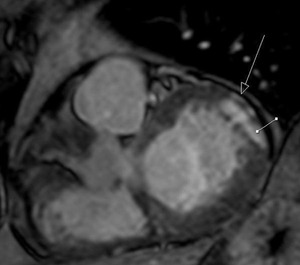
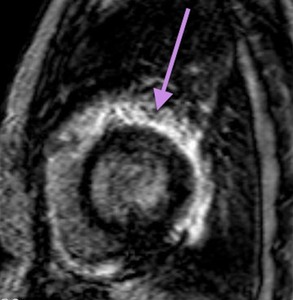
Myopericarditis, Triple-IR T1-weighted, after IV gadolinium administration....

Fig. 34:
Myopericarditis. STIR short axis image. Increased signal in the subepicardial,...

Fig. 35:
Patient with SLE and repeated episodes of pericarditis. 4-chambers viability...

Fig. 36:
Patient with SLE and repeated episodes of pericarditis. Viability study image,...

Fig. 37:
Patient with AMI. Cine T2 image, short axis. The arrow indicates small...

Fig. 38:
Viability study image, short axis. Patient with acute myocardial infarction...

Fig. 39:
Patient with a lymphoma treated with radiotherapy.
Black-blood T1-weighted MR...

Fig. 40:
Patient with a lymphoma treated with radiotherapy. Viability study image, after...

Fig. 41:
Patient with operated congenital heart disease. T1-weighted image, coronal....

Fig. 42:
Patient with operated congenital heart disease. T1-weighted image, coronal....
")
Fig. 43:
Patient with a history of thymoma treated with surgery and radiotherapy 11...
")
Fig. 44:
Patient with a history of thymoma treated with surgery and radiotherapy 11...
")
Fig. 45:
Patient with a history of thymoma treated with surgery and radiotherapy 11...
")
Fig. 46:
Patient with a history of thymoma treated with surgery and radiotherapy 11...
")
Fig. 47:
Patient with a history of thymoma treated with surgery and radiotherapy 11...
")
Fig. 48:
Patient with a history of thymoma treated with surgery and radiotherapy 11...

Fig. 49:
T1-weighted MR image, axial. Marked pericardial thickening in patient with a...

Fig. 50:
T1-weighted MR image,coronal. Marked pericardial thickening in patient with a...

Fig. 51:
Chronic constrictive pericarditis. Pericardial thickening with calcifications....

Fig. 52:
Chronic constrictive pericarditis. Pericardial thickening with calcifications....

Fig. 53:
Chronic constrictive pericarditis. Pericardial thickening with calcifications....

Fig. 54:
Chronic constrictive pericarditis. Pericardial thickening with calcifications....

Fig. 55:
Constrictive pericarditis. Pericardial thickening with calcifications....

Fig. 56:
Constrictive pericarditis. Pericardial thickening with calcifications. Patient...

Fig. 57:
Pericardial window was performed. Postsurgery T1-weighted MR image. Persist...

Fig. 58:
Cine T2-weighted image, 4 chambers. Marked dilatation of the atria. Marked...

Fig. 59:
T2-weighted cine, short axis. Patient with constrictive pericarditis....

Fig. 60

Fig. 61

Fig. 62:
Recurrent pericarditis. T2-weighted cine, 4 chambers. Mild diffuse pericardial...
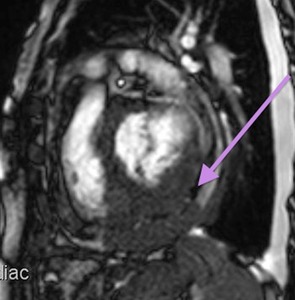
short axis, b)four chamber.
Pericardial lipoma with infiltration of the pericardium.
Isointense mass, similar to fat in all sequences, replacing the visceral pericardium and partially the myocardium, that displaces the parietal pericardium and deforms the ventricle.")
Fig. 63:
Black-blood T1-weighted MR image a)short axis, b)four chamber.
Pericardial...

Fig. 64:
Lymphoma. Black-blood T1-weighted with fat suppression after gadolinium IV...

Fig. 65:
Lymphoma. Viability image, short axis. Diffuse enhancement of the epicardium.

Fig. 66:
Lymphoma. T2-weighted cine, short axis. Mass infiltrating the myocardium,...

Fig. 67:
Lymphoma. Black-blood T1-weighted MR image, short axis. Mass isointense to...

Fig. 68:
Lymphoma. Black-blood T1-weighted MR image, short axis. Mass infiltrating the...

Fig. 69:
Lymphoma. T2-weight cine, at the level of the heart valves. Hypointense mass...

Fig. 70:
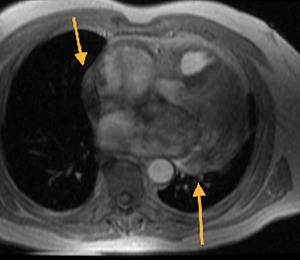
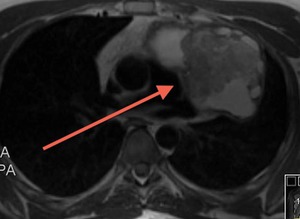
T1-weighted image, sagittal. Mediastinal mass with pericardial invasion. AP:...

Fig. 71:
T2-weighted image, sagittal. Mediastinal mass with pericardial invasion. AP:...

Fig. 72:
T2-weighted image, coronal. Mediastinal mass with pericardial invasion. AP:...

Fig. 73:
Osteosarcoma pericardial metastasis

Fig. 74:
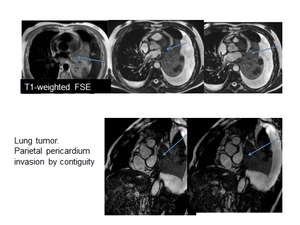
Patient with lung tumor with invasion of the parietal pleura without invasion...
.
There are invasion of the parietal pleura without invasion of the visceral pleura and pericardium.
There is no contrast enhancement.")
Fig. 75:
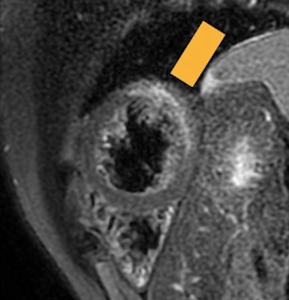
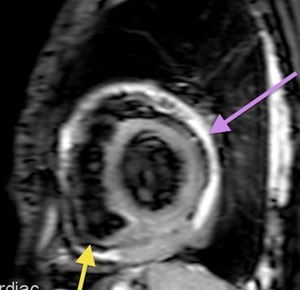
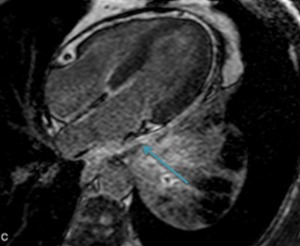
Viability image, 4-chambers shows marked contrast enhancement. Patient with...
 infiltrating the parietal pericardium. Pericardial effusion separates the visceral pericardium from the mass (yellow arrow)")
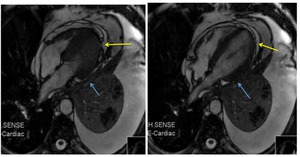
Fig. 76:
T2-weigth cine images, 4-chambers. Patient with pulmonary tumor and invasion of...