CASE 1. F/27 PALPABLE MASS in LLMQ
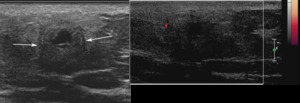
Fig.: 1.F/27 PALPABLE MASS in LLMQ - Fatty necrosis
- Irregular shape
- Partially indistinct margin
- Taller than wide
- Lack of vascularity
1. FATTY NECROSIS
- Asymptomatic or palpable
- Usually result of injury to breast fat
US findings
- Acute phase: increased echogenicity d/t edema
- Subacute phase: complex cystic phase
- Late phase (after 18months): calcified wall, thick walled or even solid
- Color Doppler
- - Internal flow increases concern for recurrent tumor
- - May see flow in granulation tissue within 6months
CASE 2. F/47 PALPABLE MASS WITH SKIN THICKENING
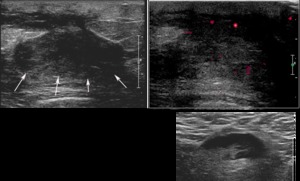
Fig.: 2. F/47 PALPABLE MASS WITH SKIN THICKENING -Diabetic mastopathy
- Partially indistinct margin
- Extending into subareolar
- Skin thickening
- Pathologic lymph node in axilla
2. DIABETIC MASTOPATHY
Clinical features
- A variant of stromal fibrosis occurring in diabetis
- Clinically hard breast
- 20yrs average interval between DM onset and mass
US
- Large poorly-defined heterogeneously hypoechoic region with indistinct margins
- No hypervascularity on color doppler
- Posterior shadowing
Differential diagnosis
- Carcinoma
- Focal or stromal fibrosis
CASE 3. F/54 SCREENING
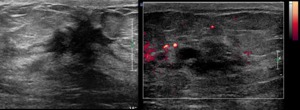
Fig.: 3. F/54 SCREENING - Fibrocystic change
- Spiculated or microlobulated margin
- Taller than wide
- Irregular shap
3. FIBROCYSTIC CHANGE
Histopathology
- Histopathologic Dx : Constellation of cysts, fibrosis and adenosis
- Spectrum of normal variation
Clinical features
- Most common Sx: mastalgia, particularly in outer portions of breasts
- Most common in pre-menopausal women; changes usually lessen in post-menopausal women
- Focal, regional or diffuse
- Increase in cyst formation in postmenopausal woman on HRT, especially estrogen alone
Radiologic findings
- Scattered echogenic foci due to calcifications
- Simple cysts
- Complicated cysts
- Clustered microcysts
- Complex cystic and solid masses
- -Often difficult to distinguish from malignancy
- Discrete masses due to fibrosis
- -Can appear irregular with shadowing
- -Often require biopsy
CASE 4. F/36 NONPALPABLE MASS on US
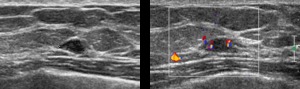
Fig.: 4. F/36 NONPALPABLE MASS on US - Adenosis
- Angular margin
- Heterogeneous echogenicity
4. ADENOSIS, SCLEROSING ADENOSIS
- Proliferation of glandular elements (lobules and ductules)
- Hyperplastic lobules contain numerous acini
- may represent failure of involution of lactational changes
- Focal or diffuse
- M/C in pre- and perimenopausal women
- Sclerosing adenosis: fibrosis of surrounding supportive stromal tissue may trap galnds
- Distorted, narrowed glandular elements
Radiologic findings
- Best diagnostic clue: microcalcifications
- -Clustered or scattered, amorphous or punctate
- Less common: oval circumscribed mass with or w/o calcifications
- -Size: usually small (12-25mm)
- -Indistinguishable from malignancy
- -Spiculated or indistinct margins, distortion
- Radiologic-pathologic discordance may necessitate excision
CASE 5. F/42 PALPABLE LESION
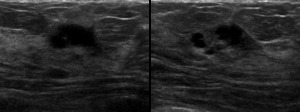
Fig.: 5. F/42 PALPABLE LESION - Ruptured inflammed cyst
- Clusterd cystic lesions with internal echogenicity
5. RUPTURED INFLAMMAED CYSTS
- Histologic Dx: inflammatory cells surrounding cyst wall and /or cyst contents
US findings
- Indistinct cyst wall in context of multiple simple cysts
- Thick walled cystic mass : complex cystic mass
- Contents : anechoic - hypoechoic tumefactive debris
- Posterior enhancment
- Indistinct margin: most common
- Fluid-debris level
MR
CASE 6. F/44 with RMRM

Fig.: 6. F/44 RMRM - Chronic inflammation
- Elongated tubular structure
CASE 7. F/46 PALPABLE MASS
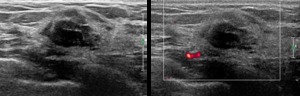
Fig.: 7. F/46 PALPABLE MASS - Chronic inflammation
- Lobulated margined, mixed-echoic nodule
CASE 8. F/32 LT.PALPABLE MASS
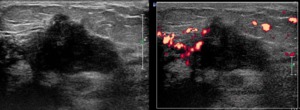
Fig.: F/32 LT.PALPABLE MASS - Acute inflammation with abscess
- Irregular mass with ill defined margin extending into the periareolar ducts
- Surrounding tissue is edematous with increased vascularity
6-8. INFLAMMATION WITH ABSCESS
- Localized pus collection within the breast tissue
- Tender palpable mass near nipple
- US findings
- Hypoechoic mass with heterogeneous texture
- Complex cystic solid mass with thick wall or septation
- Fluid-debris level
- Movement of echogenic prulent materilas
- Hyperemia in surrounding tissue
CASE 9. F/36 HARD PALPABLE MASS in LT.BREAST
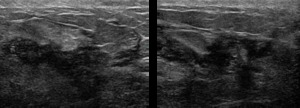
Fig.: 9. F/36 HARD PALPABLE MASS in LT.BREAST - Granulomatous mastitis
CASE 10. F/32 NIPPLE DISCHARGE
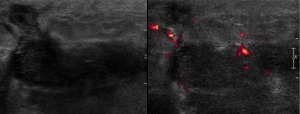
Fig.: 10. F/32 NIPPLE DISCHARGE - Granulomatous mastitis
- Large irregular shape hypoechoic mass
- Track to the skin
- Increased vascularity in surrounding tissue
9-10. GRANULOMATOUS MASTITIS
- Idiopathic mastitis, nonspecific mastitis
- Diagnosis of exclusion
- Idiopathic, probably autoimmune etiology
- Inflammatory mass with discharging sinuses
- Noncaseating granulomas
- Vast majority a/w lactation
- Typically postpartum
- Resolve on steroid therapy
Radiologic findings
- Often retroareolar
- Multiple, irregular, clustered, often contiguous, tubular hypoechoic lesions
- May be confluent
- Hypoechoic linear track to skin(cutaneous sinuses)
- Surrounding increased echogenicity due to edema
- Color doppler: hypervascularity in surrounding parenchyma
CASE 11. F/32 PALPBLE MASS in LT.BREAST
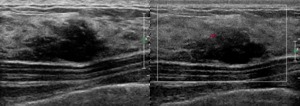
Fig.: 11. F/32 PALPBLE MASS in LT.BREAST - Fibroadenoma
- Lateral indistinct and microlobulated margin
- Hypoehoic mass with posterior shadowing
11. FIBROADENOMA
- Benign fibroepithelial tumor with mixed stromal and epithelial elements
- Most common solid mass in women under 35 yrs
- Anywhere in breast parenchyma
- Hormonally influenced growth and involution
- Vast majority self limited, involute spontaneously
- Develop on chronic cyclosporin A therapy after renal transplantation
- Highly mobile palpable painless firm mass
Radiologic findings
- Circumscribed oval or gently lobulated hypo-iso echoic mass
- Homogeneous, low internal echogenicity
- 2-4%: contain small cystic foci
- Associated calcifications
- Variable posterior enhancement
- Color doppler: Peripheral feeding vessels often visible
- Annual F/U after core biopsy showed FA
- Growth >20% in diameter in 6 months suggests possible phylloides, recommend excision
CASE 12. F/54 PALPABLE MASS NEAR AXILLA
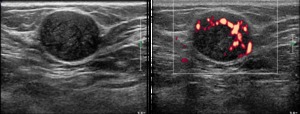
Fig.: 12. F/54 PALPABLE MASS NEAR AXILLA - Fibroadenomatous mastopathy
- Well circumscribed palpable mass with heterogeneous internal echogenicity
- Suspicious of well circumscribed malignancy or metastatic lymph node
12. FIBROADENOMATOUS MASTOPATHY
- Benign proliferative lesions
- Intermediate step(or arrested at intermediate stage) during histogenesis of fibroadenoma
- Differ from fibroadenoma as the stromal hyperplasia may not have well-defined borders and usually involves several lobules
- When palpable, mean diameter: 4cm
US
- Circumscribed lobulated mass with internal echogenic septation
CASE 13. F/43 PALPABLE MASS in RT.BREAST, s/p RECTAL CANCER
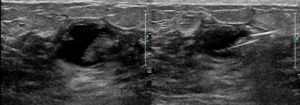
Fig.: 13. F/43 PALPABLE MASS in RT.BREAST, s/p RECTAL CANCER - Apocrine metaplasia
- Complex cystic lesion (cystic-solid)
Irregularly thick wall
- US-guided biopsy targeting for solid portion
13. APOCRINE METAPLASIA
- Dilated acini lined by columnar type secretary epithelium with granular, eosinophilic cytoplasm
- Not premalignant itself (apocrine metaplasia)
- Atypical apocrine metaplasia a/w 5.5 x relative risk of cancer
- Often associated with FCC
Radiologic findings
- Incidental new or enlarging microlobulated mass on mammography
- Incidental clustered microcysts on US
- Best diagnostic clue: clustered microcysts on US, especially if fuzzy border internally
- Size: microscopic to several centimeters
US
- Clustered microcyst
- Complete overlap with FCC
- Complicated microcyst
- Microcyst with milk-of calcium
- Clustered microcysts without a solid component do not require biopsy
