Tuberculosis of solid organs (liver, spleen, pancreas, kidney)
1. Liver and spleen
Involvement of the liver and spleen is common in miliary tuberculosis is and found in 80-100% of autopsied patients. However, it is usually in a fine miliary pattern and most of the time below the resolving capacity of CT [4]. Hepatosplenic tuberculosis may occur either often from pulmonary or miliary tuberculosis or through portal vein from GI lesions. This explains that the most common presentation is non-specific hepatosplenomegaly. Hepatosplenic tuberculosis develops under micro- or macronodular forms.
Splenic lesions may be the only sign of tuberculous involvement. In these cases lymphoma should be kept in mind in the differential diagnosis. Splenic involvement is common among HIV-positive patients. Splenomegaly in the miliary type appears as homogeneous splenic enlargement on US which is non-specific. Macronodular splenic involvement occurs in 15% of cases with HIV positivity [5].
¢ Macronodular form (Fig.1)
- rare
- pseudotumor or tuberculoma
- hypodense small mass with minimal peripheral contrast enhancement
- US:multiple hypoechoic and occasionally hyperechoic nodules
- MRI; hypointense nodule with a hypointense rim on T1-weighted images, and isointense or hyperintense nodule with a less intense rim on T2-weighted images
- early lesion : similar to an abscess
advanced lesions : similar to calcification
- D/Dx : metastases, primary malignant tumor, pyogenic abscess
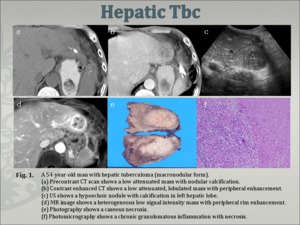
Fig.
¢ Micronodular form (Fig.2, Fig.3)
- most common and manifests usually only as moderate hepatosplenomegaly - tiny low-density foci scattered throughout the involved organs
- US: diffuse hyperechogenicity, with a bright
- D/Dx : metastases, lymphoma, sarcoidosis ,fungal infection.
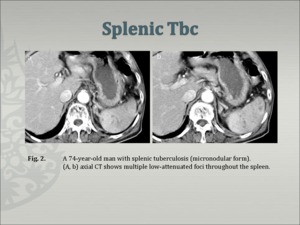
Fig.
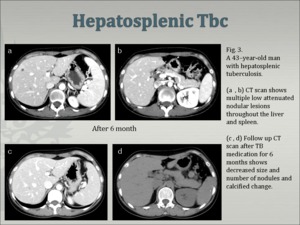
Fig.
2. Pancreas
Tuberculosis of the pancreas is extremely rare and only a few cases have been reported in the literature [6]. Although the pancreas is involved in miliary tuberculosis, it may be the only site of reactivation of tuberculosis after many years [7]. Tuberculous lesions in the pancreas are usually located in the head and less commonly in the body and tail.
Imaging findings of Pancreatic Tbc (Fig. 4)
¢ US
- Well-defined hypoechoic lesions in within an enlarged pancreatic head
¢ CT
- a focal mass within the pancreas
- low attenuation with peripheral enhancement on contrast-enhanced CT
- associated peripancreatic enlarged lymph nodes
¢ D/Dx : carcinoma of the pancreas
(chronic) pancreatitis
enlarged adjacent lymph nodes
pancreatic metastases
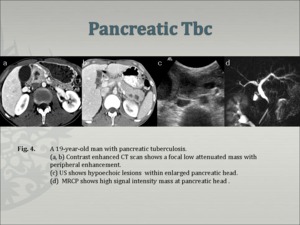
Fig.
3. Kidney
Renal tuberculosis progresses in 2 steps: (1) initial seeding and (2) reactivation.
Radiography may demonstrate calcification within the renal parenchyma. The calcification may be amorphous, granular, curvilinear, or lobar (putty kidney) [8]. Ulceration, wall thickening, and fibrosis characterize tuberculous involvement of the collecting system. Intravenous urography demonstrates a “moth-eaten” calix due to erosion on early stage, phantom calyx, Kerr kink of renal pelvis on late stage [8]. CT is helpful in identifying the manifestations of renal tuberculosis [9] (eg, calcifications). Various patterns of hydronephrosis may be seen at CT depending on the site of the stricture and include focal caliectasis, caliectasis without pelvic dilatation, and generalized hydronephrosis [8]. CT is also useful in depicting the extension of disease into the extrarenal space.
Imaging findings of Renal Tbc (Fig.5,6)
¢ Calices : dilated and filled with fluid (0-10 HU)
debris and caseation(10-30 HU)
putty-like calcification(50-120 HU)
calculi(>120 HU)
¢ Cortical thinning
¢ Parenchymal scarring
¢ Fibrotic strictures of the infundibula, renal pelvis, ureters
at contrast-enhanced CT - highly suggestive of tuberculosis
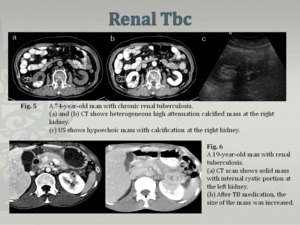
Fig.
¢ D/Dx;
chronic pyelonephritis, papillary necrosis, medullary sponge kidney, caliceal diverticulum, renal cell carcinoma, transitional cell carcinoma, and xanthogranulomatous pyelonephritis
Gastrointestinal tuberculosis
Intestinal tuberculosis is a rare manifestation of tuberculosis with unknown incidence. The incidence in hospital admissions has been reported to be 0.8% [6]; however, it is a common form of abdominal tuberculosis. Any segment of the GI tract can be involved by tuberculosis, but the ileocecal region is the most commonly involved part of the tract, noted in up to 90% of cases with intestinal tuberculosis [10]. Patients with intestinal involvement most commonly complain of diarrhea with other frequent complaints including fever, night sweats, abdominal pain and distention, anorexia and weight loss.
Pathogenesis of Gastrointestinal Tbc
Ingestion of infected material
- Formation of epithelioid tubercles in the lymphoid tissue of the submucosa (after 2–4 weeks, )
- Caseous necrosis of the tubercle - ulceration of the overlying mucosa
- Extension within the bowel wall and lymphatic spread to regional lymph nodes
- Granuloma formation, fibrosis, and scarring at late phase
Three different forms of gastrointestinal Tbc;
1. The ulcerative form
- most frequent, multiple small ulcers of 3–6 mm with irregular margin with orientation along the submucosal lymphatic structures.
2. The hypertrophic type
- less common, due to an extensive inflammatory response, resulting in a multinodular mucosal pattern, mimicking neoplastic processes.
3. The ulcero-hypertrophic pattern
- combination of both types, producing a cobblestone appearance.
Although mucosal changes are best evaluated by barium examinations, evidence of extramucosal disease is both indirect and incomplete with this technique. Ultrasound and computed tomography show extramucosal changes directly and can also occasionally pick up some mucosal changes [11]. CT also makes an important contribution in evaluating most of the complications of the intestinal tuberculosis, such as small bowel obstruction, perforation, abscess formation, fistulae, intussusception and vascular complications like bowel wall ischemia. The diagnosis is usually obtained by US- or CT-guided biopsy in most cases. The most frequent region of involvement is the ileocecal junction, followed by the ileum, cecum, ascending colon, jejunum, rest of the colon, rectum, duodenum and stomach, in descending order of frequency [3]
1. Ileocecal tuberculosis
Although tuberculosis can involve any region of the gastrointestinal (GI) tract, in about 90% of cases it affects the ileocecal valve, and the adjacent ileum and colon so the radiographic appearance of the valve was considered an important indicator of the presence of tuberculous infection[12].
Imaging findings of Ileocecal Tbc [10] (Fig. 7, 8)
¢ Barium study
- Thickening of the ileocecal valve
- Fleischner sign : wide gaping of the valve with narrowing of the terminal ileum
- Fold thickening, contour irregularity, and skip lesions
- napkin stenosis : deformation due to fibrosis, symmetric annular stenosis and obstruction associated with shortening, retraction, and pouch formation.
- Stierlins sign : narrow and fixed terminal ileum with rapid emptying of the diseased segment through a gaping ileocecal valve into a shortened, rigid, obliterated cecum
¢ US - uniform and concentric bowel wall thickening, ulceration, ascites, lymphnodes
¢ CT
- Circumferential wall thickening in the cecum and terminal ileum with associated mesenteric lymphadenopathy.
- Asymmetric thickening of the ileocecal valve and medial wall of the cecum, exophytic and engulfing the terminal ileum
- Pericecal or mesenteric fat shows either absence or minimal haziness [3]
- Associated lymphadenopathy; central areas of low attenuation ( caseous necrosis )
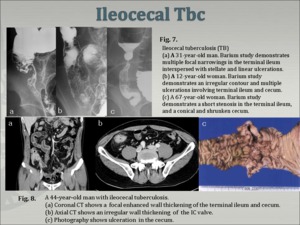
Fig.
- DDx. of ileocecal Tbc (Fig.9) - Crohn's disease (Fig. 10),Behcet's disease (Fig.11),lymphoma, amebiasis, carcinoma, and even sarcoidosis [11]. Radiological differentiation of early-stage ileocecal tuberculosis from Crohn's disease and lymphoma is usually impossible; however, the CT features of advanced ileocecal tuberculosis are not compatible with Crohn's disease and unusual for ileocecal lymphoma [10]. Computed tomography is accepted to be capable of identifying changes in the bowel wall and mesentery, which provide some differentiating factors between intestinal tuberculosis and Crohn's disease.
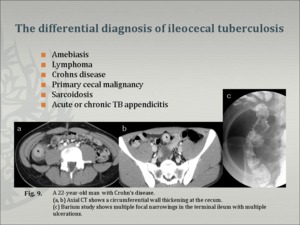
Fig.
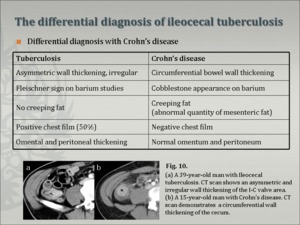
Fig.
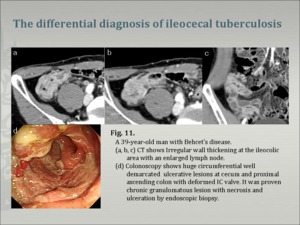
Fig.
2. Other sites of intestinal Tbc
1. TB of the esophagus (Fig. 12) ; rare in immunocompetent patients, more commonly seen in AIDS patients. Esophageal involvement usually manifests as extrinsic compression with displacement or narrowing due to adjacent lymphadenopathy most frequently at the level of the carina. With progression there are ulceration and fistula formation. Chronic fibrotic changes result in traction diverticula and strictures. Computed tomography is a more reliable method to determine full extent of the disease into mediastinum [13].
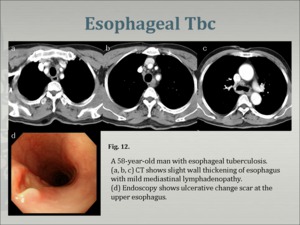
Fig.
2. TB of the stomach
; very rare, spreads from adjacent lymph nodes or via the hematogenous, antrum and distal body are usually involved. Gastric tuberculosis should be differentiated radiographically from gastric carcinoma, non-Hodgkin's lymphoma, syphilis, and sarcoidosis [14,15]. Endoscopic biopsy is indicated to obtain the diagnosis.
3. Duodenal Tbc
; occurs in only 2% of patients with GI tuberculosis, usually involves the third or fourth portion. Duodenal obstruction is presented with narrowing and sometimes fistula due to adjacent lymph nodes. A matted mass containing enlarged lymph nodes and thickened mesenteric root is demonstrated by US or CT [14].
4. TB of jejenum and ileum
; isolated involvement, occurs infrequently, usually associated with peritonitis. Imaging characteristics are nonspecific.
5. Colonic Tbc [11]. (Fig.13)
- isolated TB colitis occurs in 9% of intestinal TB, usually one segment of the colon, pancolitis is unusual and is difficult to differentiate from ulcerative colitis.
- Short or long segment (more than 5 cm) involvement can occur
- Short segment involvement usually around the hepatic flexure.
- circumferential wall thickening, narrowing of the lumen and ulcerations.
- Marked shortening and distortion of the colon can occur in advanced disease.
- The CT findings of the affected segment includes circumferential wall thickening, narrowing of the lumen and ulcerations.
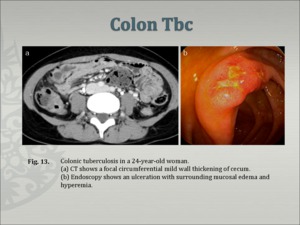
Fig.
Tuberculous peritonitis
Tuberculous peritonitis follows hematogenous spread from near or remote active primary sites or discharge of caseous material from diseased lymph nodes, intestinal segment, or fallopian tubes [3].
Three different types of tuberculous peritonitis (Fig. 14, Fig. 15) "wet-ascitic type"; 90%, large amounts of free or loculated ascitic fluid
"fibrotic-fixed"; omental involvement, matted loops of bowel and mesentery,
“dry-plastic"; unusual type and characterized by caseous nodules, fibrous peritoneal reaction, and dense adhesions [3,11,14].
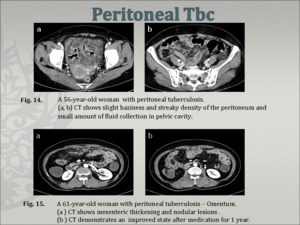
Fig.
Imaging findings of Peritoneal Tbc
¢ Ascites; Fluid with high attenuation values on CT
Ultrasound enables delineation of multiple, thin, and mobile septa and debris in the ascites [16].
CT; (25–45 HU, high protein and cellular content)
MRI; The enhancement of ascites obtained 15-20 min after intravenous administration of Gd-DTPA is not an uncommon finding in exudative ascites [17].
¢ Peritoneum
- Diffuse, regular, echo-poor peritoneal thickening of 2-6 mm or irregular thickening with tiny nodules less than 5 mm are demonstrated on US.
- smooth, slight peritoneal thickening and/or pronounced enhancement in the presence of ascites on CT.
- On MRI, a thickened omentum with ascites
¢ Omentum – nodular smudged or caked appearance
¢ Mesentery- mesenteric thickening, loss of the normal mesenteric configuration and nodular lesions, consisting of micro- (<5 mm) or macronodules (>5 mm), lymph nodes, or abscesses[17]. Diseased mesentery is shown by its increased vascularity and thickened strands within it, bunching together due to inflammation with tethering of bowel loops, forming an abdominal mass.
Bowel loops - fixed by a radiating thickened mesentery (“stellate appearance”) on CT
¢ DDx : peritoneal carcinomatosis, mesothelioma,
nontuberculous peritonitis, and lymphoma.
1. TB Peritonitis
- extension of the inflammation into the extraperitoneal compartment
- presence of a smooth peritoneum with minimal thickening and pronounced enhancement
- presence of mesenteric macronodules, relative regularity of infiltrated omentum, lymph nodes with low-density center or calcification, and splenic lesions; suggest Tbc.
2. Peritoneal carcinomatosis (Fig. 16)- nodular implants and irregular peritoneal thickening
3. Mesothelioma
- the ascites is disproportionately minimal in relation to the degree of tumor dissemination.
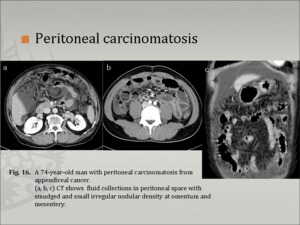
Fig.
Tuberculous lymphadenitis
Lymphadenopathy (Fig. 17, Fig. 18)is the most common finding in patients with abdominal tuberculosis. The lymph nodes are either discrete or appear as matted conglomerate masses. Enlarged nodes usually contain central hypoechoic areas [14]. Lymph node calcifications may be present in some patients.
Despite considerable bulk of adenopathy in some patients, urinary and GI obstruction has not been reported; however, biliary obstruction may occur secondary to direct ductal compression by infected nodes in association with periductal inflammation and stricture [18].
¢ the nodes display non-specific low or soft tissue attenuation values on non-enhanced scans.
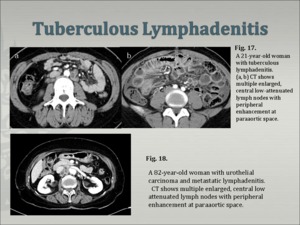
Fig.
¢ pattern of contrast enhancement is variable
- Peripheral enhancement with a low-attenuation center
: m/c (up to 60%)
- Heterogeneous, homogeneous, or absent enhancement
- Larger nodes may have a multilocular appearance
- In the healing stage, fibrosis, calcification
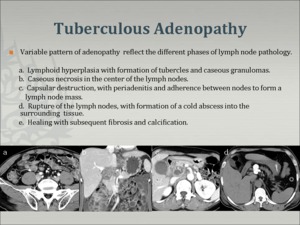
Fig.
¢ Differential diagnosis
metastatic malignancy from testicular tumors, carcinoma of the ovaries or gastrointestinal tract, and lymphoma
benign - Crohn’s disease, sarcoidosis, Whipple’s disease, and Castleman’s disease
Genitourinary tract
Tuberculosis may involve the genitourinary tract as a secondary site following hematogenous dissemination from the lungs and urogenital tuberculosis accounts for approximately 30% of cases of extrapulmonary tuberculosis[19].
The disease then spreads distally by seeding through the urothelial submucosa and lymphatic vessels to the infundibula, renal pelvis, ureter, and urinary bladder. The urothelium becomes inflamed, edematous, and ulcerated with multiple tiny granulomas in the mucosa and submucosa. The areas most severely affected are sites of anatomic narrowing, such as the infundibula of the calyces, the pelviureteric junction, and the ureterovesical junction[19].
1. Ureter (Fig. 19)- thickening of the ureteral wall and periureteral inflammatory changes
- Wall calcifications
D/Dx
ureteral stones and calcifications caused by schistosomiasis.
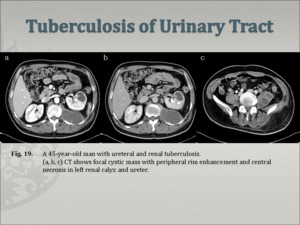
Fig.
2. Bladder
- a shrunken bladder with wall thickening
- diminutive and irregular (thimble bladder)
-DDx.- schistosomiasis, cytoxan cystitis, radiation-induced bladder calcification, calcified bladder carcinoma, and encrusted foreign materials, transitional cell carcinoma.
-
3. Adrenal Glands
Adrenal involvement in tuberculosis is rare. It may manifest as unilateral or bilateral adrenal masses with central areas of necrosis .
Adrenal atrophy with calcification
May present with Addison disease [20].
4. Female genital organs
- almost always involves the fallopian tubes in women (94% of cases)
- usually causing bilateral salpingitis
- at hysterosalpingography are always abnormal,
with obstruction and multiple constrictions of the fallopian tubes
endometrial adhesions or deformity of the cavity
- Salpingitis caused by hematogenous dissemination is almost always bilateral. (Fig. 20)- A tubo-ovarian abscess that extends through the peritoneum into the extraperitoneal compartment suggests tuberculosis.
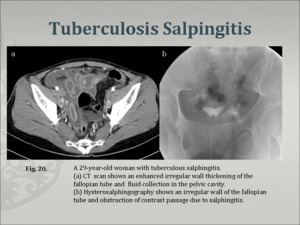
Fig.
5. Male genital organs
- Tuberculous involvement of the prostate gland or seminal vesicles may lead to necrosis, calcification, caseation, and cavitation [18]. Tuberculous epididymo-orchitis usually manifests at ultrasonography as focal or diffuse areas of decreased echogenicity with epididymal involvement [8].

















