ECR 2010 / C-1658
A pictorial review of the imaging findings in abdominal tuberculosis
Congress:
ECR 2010
Poster Number:
C-1658
Type:
Educational Exhibit
Keywords:
Gastrointestinal tract
Authors:
A. L. Williams1, H. Stockley2, R. Filobbos3; 1Wirral/UK, 2Preston/UK, 3Manchester/UK
DOI:
10.1594/ecr2010/C-1658

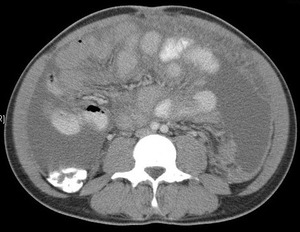
Fig. 1:
Contrast enhanced CT shows gross coeliac and retroperitoneal lymphadenopathy...
. References: R Filobbos; Radiology, North Manchester General Hospital")
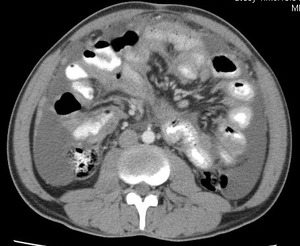
Fig. 2:
Contrast enhanced axial CT to illustrate grossly enlarged and low attenuation...
. References: R Filobbos; Radiology, North Manchester General Hospital")
Fig. 3:
Coronal reformat to illustrate grossly enlarged and low attenuation...

Fig. 4:
Contrast enhanced CT scan shows dense ascites, thickened enhancing peritoneum...

Fig. 5:
Contrast enhanced CT scan shows dense ascites, thickened enhancing peritoneum...

Fig. 6:
Contrast enhanced CT scan shows dense ascites, thickened,enhancing peritoneum...
. References: R Filobbos; Radiology, North Manchester General Hospital")
Fig. 7:
Contrast enhanced axial CT which shows perihepatic chylous ascites with fat...
. References: R Filobbos; Radiology, North Manchester General Hospital")
Fig. 8:
Contrast enhanced axial CT shows thickening and enhancement of the medial...
. References: R Filobbos; Radiology, North Manchester General Hospital")
Fig. 9:
Axial contrast enhanced CT image of a patient with thickened medial aspect of...

Fig. 10:
Endoscopic findings of patient in Figs 8 & 9 which shows mocosal thickening of...

Fig. 11:
Barium follow through demonstrating grossly abnormal terminal ileum and caecum...

Fig. 12:
Transverse ultrasound image depicting marked mural thickening of the ileocaecal...

Fig. 13:
Transvaginal ultrasound image demonstrating a markedly thick walled terminal...

Fig. 14:
Transverse ultrasound image demonstrating a markedly thick walled caecum with...
. References: R Filobbos; Radiology, North Manchester General Hospital")
Fig. 15:
Axial T2 weighted small bowel MR enterography image shows thickening of the...
. References: R Filobbos; Radiology, North Manchester General Hospital")
Fig. 16:
Axial post contrast T1 weighted small bowel enterography image shows...
. References: R Filobbos; Radiology, North Manchester General Hospital")
Fig. 17:
Contrast enhanced CT shows gross circumferential wall thickening of the jejunum...
. References: R Filobbos; Radiology, North Manchester General Hospital")
Fig. 18:
Contrast enhanced CT shows gross wall thickening and luminal narrowing of the...
. The patient was severely immunocompromised with HIV infection and subsequently died. References: R Filobbos; Radiology, North Manchester General Hospital")
Fig. 19:
Contrast enhanced CT shows marked thickening of the small bowel folds in a...

Fig. 20:
Contrast enahnced CT shows marked small bowel wall thickening and luminal...
. References: R Fillobbos; Radiology, North Manchester General Hospital")
Fig. 21:
Contrast enhanced CT shows splenomegaly and multiple low attenuation foci in a...
. References: R Filobbos; Radiology, North Manchester General Hospital")
Fig. 22:
Axial contrast enahnced CT Thorax on mediastinal windows shows muliple enlarged...
. References: R Filobbos; Radiology, North Manchester General Hospital")
Fig. 23:
Contrast enhanced CT Thorax which shows evidence of soft tissue density miliary...

Fig. 24:
Contrast enhanced CT shows multiple low attenuation foci in the spleen. Note...
 and spleen (micronodular) and multiple enlarged low attenuation necrotic retroperitoneal nodes. References: R Filobbos; Radiology, North Manchester General Hospital")
Fig. 25:
Contrast enhanced coronal reformat shows multiple low attenuation foci in both...

Fig. 26:
Ultrasound of the spleen shows multiple small hyperechoic foci consistent with...

Fig. 27:
Contrast enhanced axial CT which shows focal hypoattenuating lesion in the...

Fig. 28:
Contrast enhanced axial CT shows bilaterally enlarged heterogenous adrenal...

Fig. 29:
Contrast enhanced coronal reformat of same patient in Fig 28 shows bilaterally...

Fig. 30:
Longitudinal ultrasound image of the right kidney shows hydronephrosis and...
. References: R Filobbos; Radiology, North Manchester General Hospital")
Fig. 31:
Contrast enhanced oblique coronal CT in same patient as Fig 30. Shows...

Fig. 32:
Transverse ultrasound image of the right kidney demonstrating a dilated upper...

Fig. 33:
Longditudinal ultrasound image of a kidney demonstrating calyceal dilatation...

Fig. 34:
Contrast enhanced CT shows multiloculated pelvic mass with enhancing wall. This...
. References: R Filobbos; Radiology, North Manchester General Hospital")
Fig. 35:
Contrast enhanced CT shows necrotic coeliac node in a patient with a...
. References: R Filobbos; Radiology, North Manchester General Hospital")
Fig. 36:
Contrast enhanced CT shows necrotic ileocolic node in a patient with a...
 References: R Filobbos; Radiology, North Manchester General Hospital")
Fig. 37:
Contrast enhanced axial CT shows right tuberculous psoas abscess and enlarged...
 shows right tuberculous psoas abscess and enlarged necrotic retroperitoneal nodes. References: R Filobbos; Radiology, North Manchester General Hospital")
Fig. 38:
Contrast enhanced coronal reformat (same patient as Fig 2, 3, 7 & 37) shows...