Purpose
CNS tuberculosis is a leading cause of morbidity and mortality in developing countries, caused by Mycobacterium tuberculosis. There is further worsening of the scenario even in developed countries due to increasing numbers of HIV infected patients. Classical presentation of CNS tuberculosis poses no problem for clinicians. However, giant tuberculomas and solitary ring enhancing lesions present as diagnostic challenge because they simulate many infectious and non-infectious medical conditions. The purpose of our scientific exhibit is:
- Highlights the characteristic imaging features of CNS tuberculosis
- Emphasis on giant tuberculomas and solitary ring enhancing lesion in typical and atypical locations which mimic other pathologies
- Introducing a new sign “outer rim excrescence sign’ in ring and/or solid enhancing lesions as a differential point
Material and methods
This retrospective study includes 21 patients of either surgically or clinically (mainly response to ATT) proven CNS tuberculosis. These patients presented with varied clinical features such as fever, headache, nausea, vomiting, photophobia, cranial nerve palsies, limb weakness and altered sensorium with signs & symptoms localized to the topographic location of tuberculomas. There were 13 male and 8 female patients with age range between 9 to 70 years (Mean age- 30years). Imaging was performed either with MDCT, MRI or both. Routine pulse sequences were obtained. Only five patients had active tubercular focus elsewhere in the body. None of the patients was immunocompromised. Three patients underwent surgery, whereas in rest of the patients the diagnosis was confirmed with response to ATT.
Qualitative analysis:
Morphological features of solid enhancing, ring enhancing and giant tuberculoma were described in T1W and T2W images on the basis of signal intensity. Presence of more than one lesion was considered as ‘multiple’ and solid enhancing lesion of more than one cm. size was considered as ‘giant tuberculoma’. Irregularly marginated enhancing projection from the outer wall of ring enhancing and/or solid lesions was described as ‘outer rim excrescence sign’. Other classical findings of CNS tuberculosis like multiplicity of lesions, enhancing exudates, leptomeningeal enhancement, focal cerebritis and infarct were taken into consideration for making the diagnosis.
Pathophysiology:
There is hematogenous spread of tubercle bacilli to CNS which may be primary or more commonly secondary to infection elsewhere in the body. Rupture of Rich focus (focus of infection) in subpial or subependymal region gives rise to generalized bacillimia in subarchnoid space and CSF. Meningitis is the most frequent manifestation of CNS tuberculosis; however incidence of other manifestations keeps on increasing which includes tubercular granuloma, abscess, cerebritis, pachymeningitis, spondylodiscitis and spinal arachnoiditis.
Results
Solitary tuberculomas (ring or solid) were seen in seven patients which were located in pons(2), basal ganglia(1), parietal lobe(2), temporal lobes(1) and cord parenchyma(1). Four patients showed presence of 2 to 3 lesions and one of the lesions was categorized as giant tuberculoma. Smaller solid or ring enhancing lesions with giant tuberculoma enforces the correct diagnosis. Multiple lesions with other associated findings were noted in nine patients. Pure calvarial involvement was noted in one patient only. Total 17 patients showed solitary or multiple ring enhancing lesions. Five patients showed solid enhancing lesions (giant tuberculoma). Outer rim excrescence sign was noted in a total of nine patients. One case of tubercular abscess was noted involving the pons in an 11 year male patient. Both brain and spinal tuberculosis was noted in 3 patients. Only two patients presented with meningitis and hydrocephalous which is considered as the most common manifestation in the literature.
Table 1
Contrast characteristics | T1 | T2 | Patho-physiology |
Ring enhancing n=17 | Centre-hypointense Periphery-hyper | Centre-hyperintense Periphery-hypo/iso Outer rim-hyper | Granuloma with central liquefaction |
Solid enhancing (size<1 cm) n=8 | Isointense | hyperintense | Non-caseating granuloma |
Solid Enhancing (size>1cm) n=5 | Iso- to hypointense | Profoundly hypo with Punctate hyperintense foci | Caseating solid granuloma |
Outer rim excrescence n =9 (Enhancing outer projection from solid or ring enhancing lesion ) | Indistinguishable from perilesional edema | Indistinguishable from perilesional edema | Unknown (?Granulomatosis vaculitis in surrounding parenchyma) |
DISCUSSION
Cases of atypical presentation of CNS tuberculosis clinically and on imaging keeps on increasing in Indian subcontinent which appears to be most serious form of the infection and responsible for high mortality and morbidity. Pandemic of AIDS further worsens the disease. Apart from the typical cases of CNS tuberculosis, single or multiple tuberculomas, especially solitary ring enhancing lesion and giant tuberculomas are major diagnostic challenge with unusual locations and symptoms.
Classical presentation of CNS tuberculosis:
Majority of patients of CNS tuberculosis show multiple discrete or conglomerate ring enhancing and solid enhancing lesions in almost every region of the brain (Fig 1) which is usually associated with enhancing exudates in basal and suprasellar cisterns, hydrocephalous with ventricular ependymal enhancement, focal to diffuse leptomeningeal enhancement, tubercular abscess, focal cerebritis and infarcts. Usual clinical signs and symptoms are present in such patients. Active focus of tuberculosis is not always noted elsewhere in the body.
Meningitis
Tuberculous meningitis is the most common manifestation of CNS tuberculosis. In our study, meningitis was seen in two patients only. Hematogenous seeding of the meninges or release of bacilli into the meningeal space is the likely etiology. Imaging is not always helpful in diagnosis of meningitis. Diagnosis is made by CSF analysis and carefully observed clinical signs and symptoms. PCR of CSF is more sensitive and confirmatory in comparison to AFB culture. MRI is superior to CT in early detection of the meningeal pathology. Thick and nodular meningeal enhancement, enhancing basal exudates especially in basal and suprasellar cisterns, hydrocephalus and focal infarct secondary to vaculitis are commonly observed findings (Fig 2). Ring or conglomerate enhancing lesions may or may not be present (Fig 3).
Intracranial tuberculomas:
These are the most severe and dangerous form of CNS tuberculosis. Tuberculomas may be single or multiple and can be seen anywhere in the brain. The variable histological morphological features determine their imaging characteristics. Different forms of tuberculomas can be seen in single patient. Histologically, tuberculomas are categorized as noncaseating, caseating solid and caseating granuloma with central liquefaction. Their signal characteristics on MR imaging has been described in table 1. They are commonly encountered without evidence of a previous or concomitant infective focus elsewhere in the body. Multiple tuberculomas with concomitant findings facilitate the diagnosis.
However, solitary ring enhancing or giant solid enhancing tuberculomas pose major diagnostic challenge in present scenario (Fig 4). Cases of solitary tuberculoma had increased substantially in developing countries, especially in children. They are usually located in deeper region of the brain like basal ganglia, thalamus and brainstem and simulate other infectious and non-infectious diseases of brain. Such patients usually present with unusual signs and symptoms. Symptoms are often limited to seizures and mass effect, as it is usually associated with moderate to massive perilesional edema. Early recognition of such tuberculomas is of paramount importance as judicious use of ATT can have a dramatic effect and prevent unnecessary surgical intervention and its morbidity and mortality.
Solid giant tuberculomas:
Histological they are composed of solid caseating or non-caseating granuloma. In our study the tuberculoma was considered giant if its size exceeds one cm.Usually they are solitary, however sometime may be accompanied by sub centimeter ring or solid enhancing lesions. Its T2 wt signal is quite characteristic, depicting profoundly hypointensity.T1 wt image shows either iso or hypointense signal. There is intense and homogenous contrast enhancement in gadolinium enhanced T1 wt images (Fig5, Fig, 6, Fig 7).Perilesional edema is significant in majority of the cases.
Solitary ring enhancing lesion (Granuloma with central liquefaction):
Single ring enhancing lesion is a common imaging finding in endemic regions, especially in children and young adults presenting mostly with seizure activity without any constitutional signs and symptoms. Differential diagnosis covers a long list of pathologies (Fig 4). Neurocysticercosis (NCC) is main simulating entity in Indian subcontinent. Both NCC and tubercular ring enhancing lesion involve any part of the brain including basal ganglia, thalamus and brainstem. Imaging findings have been described to differentiate NCC from tuberculoma; however it lacks sensitivity and specificity. Here, we introducing a new sign ‘outer rim excrescence sign’ (Fig: 8) to differentiate tuberculoma from other ring enhancing lesions, however further comprehensive study is required for confirmation. This is defined as irregularly marginated enhancing projection from the enhancing ring into the surrounding parenchyma. Its T1 and T2 characteristics are indistinct from adjacent perilesional edema. We postulate the granulomatous vaculitis in surrounding parenchyma as most probable causative factor. We observed the outer rim excrescence sign in total nine patients.
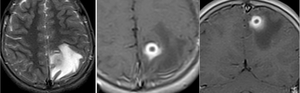
Fig.: Fig 8, A-C: An 11 year male patient presented with seizure and non-specific headache (Solitary Ring enhancing lesion).
Fig 8, A: T2wt axial image shows thick rim of slight hyperintensity with central hypointensity and ill-defined peripheral hypointensity surrounded by hyperintense edema.
Fig 8, B-C: Gadolinium enhanced T1 wt images show thick ring enhancement with enhancing projection into the perilesional parenchyma outside the enhancing thick rim (Outer rim excrescence sign)
Spinal tuberculosis:
Pathophysiology of spinal tuberculosis is the same as tubercular meningitis. Imaging findings include ring or conglomerate enhancing intramedullary lesions, myelitis, arachnoiditis, focal or diffuse leptomeningeal enhancement, epidural abscess, spondylodiscitis, infarction and syringomylia. Most common presentation is spondylodiscitis which is usually associated with pre/paraspinal and epidural collection.
Intramedullary tuberculoma is rare even in endemic regions. However, due to increasing use of MRI, detection of such lesions is increasing. MRI facilitates the better delineation and characterization of lesion and further management and treatment response. The MRI appearance of intramedullary tuberculoma are characterized by fusiform swelling of cord, hypo –to isointense signal on T2wt image with surrounding hyperintense edema, so to hyperintense foci in T1 wt image which show ring and / or conglomerate enhancement.
CONCLUSION
- Classical imaging findings pose no problem for diagnosis of CNS tuberculosis
- Cases of giant or solitary ring enhancing lesions keep on increasing which mimic other infectious and non-infectious pathologies
- Atypical clinical signs and symptoms are not unusual
- High index of clinical suspicion is required for diagnosis
- Profound T2W hypointensity is reliable predictor for giant tuberculomas with intense contrast enhancement, especially in deep locations
- ‘Outer rim excrescence’ sign may contribute in cases of ring and solid enhancing lesions, however it requires further comprehensive study to record as a differentiating feature
REFERENCE
- Jinkins JR, Gupta R, Chang KH, et al. MR imaging of central nervous system tuberculosis. Radiol Clin North Am 1995;33:771–86
- Gupta RK, Jena A, Sharma A, Guha DK, Khushu S, Gupta AK. MR imaging of intracranial tuberculoma. J Comput Assist Tomogr 1988;12:280–285
- Gupta RK, Pandey P, Khan EM, Mittal P, Gujral RB, Chhabra DK.Intracranial tuberculomas: MRI signal intensity correlation with histopathologyand localized proton spectroscopy. Magn Reson Imag1993;11:443–449
- Gupta RK, Kathuria MK, Pradhan S. Magnetization transfer MR imaging in CNS tuberculosis. AJNR Am J Neuroradiol 1999;20:867-75
- Gupta RK, Jena A, Singh AK, Sharma A, Puri V, Gupta M. Role of magnetic resonance (MR) in the diagnosis and management of intracranial tuberculomas. Clin Radiol 1990;41:120-7
- Trivedi R,Saksena A,Gupta RK.Magnetic resonance imaging in Central nervous system tuberulosis.IJRI/NOV2009;VOL19 :256-265
- Brismar J, Hugosson C, Larsson SG, Lundstedt C, Nyman R. Tuberculosis as a mimicker of brain tumor. Acta Radiol 1996;37:496-505
- Gupta RK, Jena A, Sharma A, Guha DK, Khushu S, Gupta AK. MR imaging of intracranial tuberculomas. J Comput Assist Tomogr 1998;12:280-5
- Kim TK,Chang KH et al.Intracranial tuberculoma:comparison of MR with Pathologic Findings.AJNR 16:OCT 1995:1903-08
- Gupta RK, Husain N, Kathuria MK, Datta S, Rathore RK, Husain M. Magnetization transfer MR imaging correlation with histopathology in intracranial tuberculomas. Clin Radiol 2001;56:656-63
- Kumar A, Montanera W, Willinsky R, TerBrugge KG, Aggarwal S. MR features of tuberculous arachnoiditis. J Comput Assist Tomogr 1993;17:127-30
- Gupta RK, Agarwal P, Rastogi H, Kumar S, Phadke RV, Krishnani N. Problems in differentiating spinal tuberculosis from neoplasm on MRI. Neuroradiology 1996;38:S97-104

. A large hypointense lesion is seen in left occipital lobe with moderate perilesional edema (caseating granuloma)
Fig1, C: T1-weighted axial image shows isointensity in above-mentioned multiple T2 hyperintense lesions and large occipital hypointense lesion.
Fig 1, D-F: Gadolinium –enhanced T1-weighted images show multiple solid, ring enhancing lesions (granuloma with central liquefaction).Focal cerebritis is noted in posterior left parietal cortex.")
: Meningitis with right thalamic infarct in a 4 year male patient
Fig 2 A: N.C.C.T axial section shows well defined hypodensity in right thalamus.
Fig 2 B, C: C.E.C.T axial sections show diffuse leptomeningeal enhancement and exudates along basal cisterns and adjacent sulci. No enhancement is seen in right thalamic hypodensity (infarct due to vaculitis")
 and sagittal (C) images show diffuse leptomeningeal enhancement, enhancing exudates, focal cerebritis and multiple ring enhancing lesions.")

, sagittal T1 (C) images show profound hypointense and isointense lesion in the medulla with moderate perilesional edema.
Fig 5, D: Gadolinium enhanced coronal (D) shows intense contrast enhancement in both lesions with multiple punctate hypointensities within it. Two small solid enhancing lesions were also noted right fronto-parietal lobes (not shown).")


 and T1 (B) Saggital images show expansile isointense and hyperintense intramedullary cord lesion respectively at D4-D5 level. High signal cord edema is noted in cranial and caudal cord in T2 sagittal image
Fig 9, C, D: Contrast enhanced sagittal (C) and coronal (D) images show conglomerate ring enhancement in expansile cord lesion with thick leptomeningeal enhancement at D4-D5 level.")
 shows diffuse intramedullary high signal in lower dorso-lumbar cord including the conus medullaris which does not show enhancement in T1 wt gadolinium Image (Fig B) consistent with tubercular myelitis.Irregular nodular enhancement is seen along the pial surface of cord with thick nodular leptomeningeal enhancement
Fig10, C, D: Coronal and axial T1wt images shows diffuse enhancement in thecal sac and clumped intrathecal nerve roots consistent with arachnoiditis. Small fluid collection is noted in right lateral recess region .")