Background
Facet syndrome has high prevalence in elderly populations,
because of their frequent arthritic degeneration of the interapophyseal joints in conditions of chronic overload,
sometimes associated with repeated microtrauma.
Less frequently facet syndrome is associated to synovitis with fluid distension of the articular capsule (which might be caused by microtrauma,
inflammatory aspecific reactions or their rheumatological involvement),
entrapment of meniscoid articular structures,
synovial impingement,
subluxation,
chondromalacia,
expansive processes and other rarer causes.
Clinical diagnosis of facet syndrome is not straightforward,
bacause of its clinical presentation,
sometimes very similar to more generic pain affections of the spine,
and also considering how often back pain is multifactorial.
Anatomy
Interapophyseal joints are established between superior and inferior articular processes of two adjacent vertebrae; they are normal diarthroses and,
thus,
are constituted by hyaline cartilage,
synovial membrane and fibrous capsule.
These joints assist the intervertebral discs in supporting the load,
restricting spine movements which could be potentially dangerous for spinal cord and nerve roots.
The orientation of the interapophyseal joints is different at each level of the spine; they present a coronal orientation,
with an angle of about 30 to 45° relative to the horizontal plane at cervical level,
they tilt to an angle of about 60° in the dorsal tract,
and are oblique sagittal at lumbar level.
Interapophyseal joints are innervated by the medial branches of the dorsal nerve roots; each joint receives double innervation by the upper and lower nerve of each level; the presence of nociceptive and autonomic fibres suggests how these joints may cause pain in case of spinal overload.
Clinical features
The most consistent symptom is median back pain,
which may radiate to the gluteal region and the posterior portion of the tight without a specific dermatomal distribution; usually,
there is no pain radiation below the knees.
Pain is often strongest in the morning and gets worse with rest,
hyperextension and twisting movements towards the affected side.
Neurological examination usually results normal.
In case of cervical facet syndrome,
patients refer about a paraspinal pain at the level of the involved joint(s),
neck pain increased by rotational movements and radiating to shoulders,
headache.
Imaging findings
Radiological study of typical facet syndrome cases shows arthritic alterations of the interapophyseal joints; acquiring radiographs in flexion-extension often shows rigidity or hypo-mobility of the involved spinal tract.
CT and MRI are useful as well to demonstrate osteo-arthritis (respectivily Fig.
1 and 2)

Fig. 1: CT scan showing osteophytes in a left interapophyseal joint at lumbar level
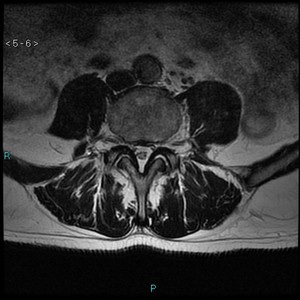
Fig. 2: MR, T2w, axial plane.
Image shows bilateral arthritis and effusion of interapophyseal joints at lumbar level.
of the interapophyseal joint,
also to highlight any asymmetric orientation of the facets.
MRI,
in cases of re-exacerbation of pain may show joint effusion (Fig.3)

Fig. 3: MR, T2W, Axial plane.
Monolateral interapophyseal joint effusion.
especially in patients with vertebral instability,
and bone edema.
When available,
upright MRI can highlight instability and slipping of the articular surfaces.
Management and Treatment
All available procedures can easily be performed under fluoroscopic or CT guidance; the choice of the used method largely depends on the preferences of the operator and local availability.
Undoubtely CT allows extremely accurate positioning,
without exposure to ionizing radiation for the operator and almost never requires intra-articular injection of contrast medium.
Two main groups of procedures can be identified to treat facet syndrome:
- Articular infiltrations
- Nerve blocks /Neurolysis
Articular infiltrations
Lumbar articular infiltrations performed under fluoroscopic guidance require lateral obliquation of the C-arm to outline the profile of the rear portion of the joint.
Usually,
a tilt angle of 30-40° from the side of the joint similar to the projection named “of the dog”,
is adequate (Fig.4).
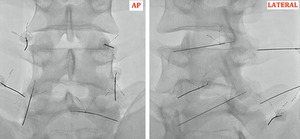
Fig. 4: Fluoroscopy (AP and Lateral Projection).
Correct placement of needles at lumbar level for interapophyseal joint infiltration.
It should be recalled that the articular space often does not lie in a plane,
but is more frequently “C- shaped”; therefore,
often,
it is not possible to outline the entire joint surface.
It is important,
thus,
that the the angle of incidence is parallel to the rear portion of the joint line.
A spinal needle (commonly 22G) is advanced towards the intra-articular or periarticular space for each joint is treated.
In case of severe joint space narrowing,
or when osteophytes tend to stop the acces to the articular space,
the needle should be directed towards the lower portion of the joint,
because in that area the synovial recess is usually accessible.
In case of intra-articular acces,
a minimum injection of contrast medium (0.1-0.3 mL) can be made,
but using an adequate radiological technique this can be unnecessary.
Once the needles are correctly placed,
a solution of 1-2 mL containing bupivacaine at 0.5% or lidocaine 2% and 20-40 mg of triamcinolone acetonide or metylprednisolone is injected; the rational of the steroids injection is that they can reduce inflammation of the synovial and periarticular strucutres; however,
it is strongly recommended not to inject a greater volume inside the articular capsule,
because it could lead to its rupture,
and also bacause its hyperdistension can be painful as well as in the case of articular effusion.
In case of para-articular approach,
the tip of the needle is placed in contact with the bone,
near to the articular space,
and the needle can be moved along the articular line,
to peform infiltrations in more points of the capsule; in this case it is never necessary to perform contrast medium injection,
and a greater amount of drugs can be overall injected.
The choice of the method to be used is sujective,
as it has not been demonstreted the superiority of one another.
Using CT guidance,
the procedure is similar and simple as well; the needle direction can be choosed following the joint anatomy (Fig.5)

Fig. 5: CT scan.
Under CT guidance two spinal needles are placed at the level of L5-S1 interapophyseal joints.
also avoiding the obstacle eventually made by osteophytes; in case a Fluoro-CT guidance is used,
this leads to greater radiation dose exposure for the operator,
but significantly quicker execution.
In each case,
a positive result to an intra-articular injection can be considered as a positive diagnostic test to determine if the referred pain is mainly caused by a facet syndrome; “responders”,
should then be treated with a different technique,
capable of more lasting results such as denervation,
using radiofrequency,
crioablation or alcohol injection.
Nerve blocks
This is a technique performed with the only aim of making a diagnostic test,
in this case once reached the level of the medial branch of the dorsal nerve root,
a volume of 0,5-1,0 mL bupivacaine or lidocaine is injected; the result of this test is considered positive if pain is significantly less intense or absent 30 minutes after the injection.
At lumbosacral level,
with fluoroscopic guidance in AP projection,
the needles are inserted directly having as a target the upper part of the junction between the transverse process and the pedicle.
With a slightly oblique approach,
it is possible to tap the lamina with the tip of the needle,
and then bend it laterally towards the transverse process; after making that,
the injection of local anesthetics is possible.
Neurolysis
These techniques are more costly than the articular infiltrations and,
thus,
should be reserved to patients who have already showed significant response to intra-articular treatment or nerve blocks.To perform neurolysis,
the anatomical approach is similar to the one used for nerve blocks,
but because of the requested extremly precise needle placement and possible complications,
it is preferable to use CT guidance.
Neurolysis can be obtained using different means,
such as injection of ethyl alcohol,
radiofrequencies or cryotherapy.
Nowadays,
alcohol is rarely used,
because its diffusion,
once injected,
is poorly controllable,
also if it has the undoubt advantage of lower cost.
Neurolysis with radiofrequency is the most widely used technique; as the procedure is sometimes quite painful,
a local anesthetic administration togheter with a mild sedation of the patient can be useful.
20G radiofrequency needles are used,
with an exposed tip of 0,5 – 1,0 cm.
Because of the physical principles of radiofrequency,
it is important that the exposed tip of the electrode is positioned as parallel as possible to the course of the nerve to be thermo-ablated.
For lumbar vertebrae up to L4,
it is possible to approach the medial branch of the dorsal berve root before its bifurcation into an upper and lower articular branch,
so as to interrupt the nerve conduction in both; this point is placed in the nip between the transverse and the articular process.
At L5 level,
it is the same dorsal branch running between the wing of the sacrum and the articular process of the sacrum itself; that anatomical point will be the target,
easily accessible via an AP projection under fluoroscopic guidance.
Once the needle is placed,
the electrode is inserted into it,
and some tests are performed before proceeding with the lysis; first,
sensitive tests such as reproduction of the pain symptoms of the patient,
and then motor tests,
to confirm good positioning of the needle tip.
Once these tests are passed,
perineural anesthesia is performed,
and at that point it is possible to proceed to neurolysis,
using a temperature of 90°C for about 60 seconds.
Newer RF generators allow to treat simoultaneously more then one level,
and allow also to make a sort of “neuromodulation” using pulsed radiofrequencies; in these cases the temperature does not exceed 42°C,
so that the nerves are not irreversibly damaged,
but only “shocked” and restore their normal functions in a few months.
