The AAS includes a heterogeneous group of patients with a clinical profile of aortic pain with a history of severe arterial hypertension.
In our case,
the diseases considered were intramural haematomas (IH),
aortic dissection (AD),
ruptured aneurysm and ulcerated plaques / aortic ulcers.
Seventy-nine per cent of all patients were male with a mean of 65 years old (range 29-99 years).
The most common symptom was pain (thoracic,
abdominal,
lumbar) followed by pulsatile mass.
There was positive correlation for AAS in 47% of the studies.
The most frequent pathology was aortic rupture (32 cases),
followed by AD type A (24%),
penetrating ulcer 24%,
15% aortic dissection type B and 5% of IH.
1.
Ruptured aneurysm of the aorta (AA).
In our series,
was the most prevalent entity,
due to the high frequency of aneurysms and chronic degenerative process that causes localized weakening of the aortic wall. The natural history is progressive expansion and rupture.
It is considered that there is an AA when the diameter of the aorta is more 3 cm or exceeds 50% of normal arterial diameter (Fig.
1).
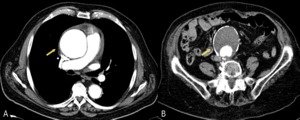
Fig. 1: Images of CT with intravenous contrast showing an ascending thoracic aortic aneurysm (image A, arrow) and abdominal aortic aneurysm with extensive mural thrombus, with no signs of complication (image B, arrow)
References: Radiology Department. Hospital Universitario La Princesa. Universidad Autónoma de Madrid (Spain)
Recall that 9% of patients over 65 years old have an AAA rupture and 15,000 deaths occur annually in the United States.
Is more prevalent in men (4:1) and the most frequent location is infrarenal (Fig.
2).
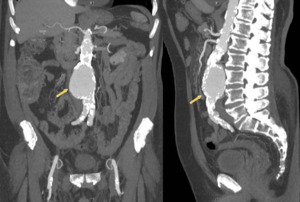
Fig. 2: MIP reconstructions showing uncomplicated infrarenal aneurysm with extensive aortoiliac atheromas (arrows).
References: Radiology Department. Hospital Universitario La Princesa. Universidad Autónoma de Madrid (Spain)
The consensus over AA of the Spanish Society of Angiology and Vascular Surgery points out that the number of AA is estimated at 250,000 cases and mortality from aneurysm rupture is between 7,000 and 8,000 cases a year in Spain.
In some cases prior to the CT angiography,
physical examination detected a painful pulsatile abdominal mass on palpation or presence of an abdominal bruit.
Rupture of an AAA occurs in one third of cases the classic triad of acute abdominal pain or back pain,
pulsatile abdominal mass,
and hypotension.
Other symptoms were renal colic,
gastrointestinal bleeding,
intestinal or lower limbs ischaemia.
The next signs are predictors of rupture:
1.
The rapid increase in the size and irregularity of the wall of the aneurysm (Fig.
3)
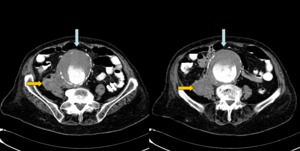
Fig. 3: Women with 85 years old. She have abdominal pain and hypotension. CT angiography was performed showing aneurysm (blue arrows), irregular posterolateral wall of the aneurysm and retroperitoneal hematoma as a sign of rupture. The patient died at surgery.
References: Radiology Department. Hospital Universitario La Princesa. Universidad Autónoma de Madrid (Spain)
2.
The discontinuity of the peripheral calcifications (Fig. 4 and Fig 5).
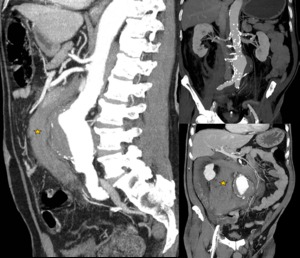
Fig. 4: A 78 year old man with abdominal pain and hypoperfusion. MIP reconstructions of aortic CT angiography with intravenous contrast showing retroperitoneal hematoma (star) with irregular calcifications in the left wall of the aneurysm, in connection with break. Emergency surgery was performed with aortoiliac bypass and the patient continues with revisions in vascular surgery department.
References: Radiology Department. Hospital Universitario La Princesa. Universidad Autónoma de Madrid (Spain)
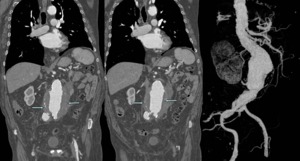
Fig. 5: A 84 year old male with abdominal pain and coronal MIP reconstructions of CT angiography aortic showing irregular wall calcification of aneurysm and small periaortic retroperitoneal hematoma. Aortic rupture was diagnosed with stent placement to current patient survival.
References: Radiology Department. Hospital Universitario La Princesa. Universidad Autónoma de Madrid (Spain)
3.
The presence of a high attenuation crescent thrombus (Fig.
6)
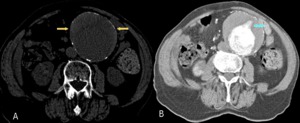
Fig. 6: Chest CT without contrast (left image) showing aneurysm of 10 cm with hyperdense mural thrombus (yellow arrows). In the right image on CT angiography, intratrombus contrast is identified as a sign of imminent rupture(blue arrow).
References: Radiology Department. Hospital Universitario La Princesa. Universidad Autónoma de Madrid (Spain)
We value as signs of breakage:
1.
High density fluid in the pericardium,
left pleural space (Fig.
7) or retroperitoneal (Fig.
8).
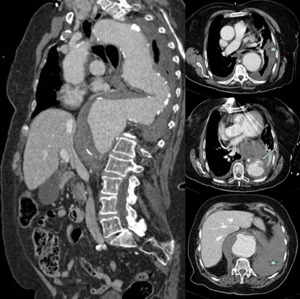
Fig. 7: Woman 81 years old with chest pain and hypotension. The chest CT angiography shows aneurysm of the aortic arch and descending thoracic aorta, with irregularity of the wall (arrow) and left hemothorax, in relation to aneurysm rupture. The patient died at surgery.
References: Radiology Department. Hospital Universitario La Princesa. Universidad Autónoma de Madrid (Spain)
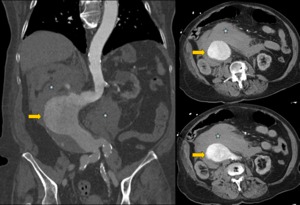
Fig. 8: Women of 89 years old with abdominal pain and lower limb lividity. In CT angiography large aortic aneurysm is identified at infrarenal abdominal aorta (arrows) with extensive retroperitoneal hematoma (star). Surgery is dismissed and the patient dies.
References: Radiology Department. Hospital Universitario La Princesa. Universidad Autónoma de Madrid (Spain)
2.
Extravasation of contrast into the mediastinum,
pleural or retroperitoneal space (Fig. 9 and Fig 10).
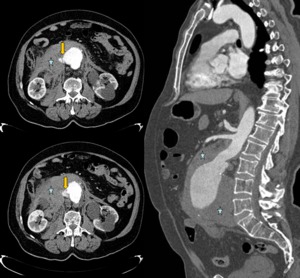
Fig. 9: A 73 years old male with abdominal pain, abdominal mass and hypotension. Axial and sagittal reconstructions of aortic CT angiography with intravenous contrast, shows abdominal aortic aneurysm, extensive retroperitoneal hematoma (stars) and presence of contrast extravasation (yellow arrows). Emergency surgery is performed with an aortoiliac graft. The patient continues to make revisions at Vascular Surgery Department.
References: Radiology Department. Hospital Universitario La Princesa. Universidad Autónoma de Madrid (Spain)
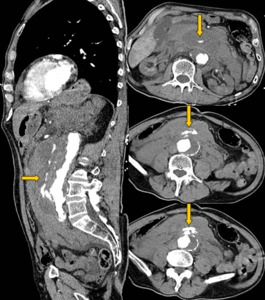
Fig. 10: A 77 year old male with acute aortic syndrome. Sagittal and coronal reconstructions of aortic CT angiography, with large retroperitoneal hematoma, ruptured abdominal aneurysm and extensive extravasation of contrast to the retroperitoneum (arrows). Aortoiliac graft is done urgently, with a fatal outcome.
References: Radiology Department. Hospital Universitario La Princesa. Universidad Autónoma de Madrid (Spain)
In our series,
we found a high prevalence in male (88.
3%) having a mean age of 75.7 years with age range between 50 and 93 years.
The incidence was 11.7% in females,
with mean age of 81.75 years and range between 72 and 85 years.
Surgery was performed in 50% of cases with aortoiliac bypass in 14 patients,
axilobifemoral (1 case),
aortobifemoral (1 case).
Mortality was very high at 73.5% of cases,
both in surgical patients and those rejected for surgery.
Three patients were used as an alternative for the endovascular repair of AA,
which was associated with less morbidity and no mortality.
Current prostheses have a self-expanding nitinol mesh or steel covered with tissue (dacron / expanded polytetrafluoroethylene or PTFE),
visible in the abdominal radiographs (Fig.
11).

Fig. 11: Abdominal X-ray showing aortoiliac stent.
References: Radiology Department. Hospital Universitario La Princesa. Universidad Autónoma de Madrid (Spain)
2.
Classic aortic dissection
Requires immediate diagnosis and treatment,
and CT angiography has a sensitivity and specificity of nearly 100% in the diagnosis.
Aortic dissection (AD) is characterized from the pathological viewpoint by passing the blood,
which penetrates the wall of the aorta through a discontinuity in the intima,
separating the intima of the media,
with variability in longitudinal and circumferential extension.
This division of the middle layer is responsible for the two most important signs for diagnosis of dissection at CT angiography:
1.
The presence of intimal flap (Fig.
12 and Fig 13)
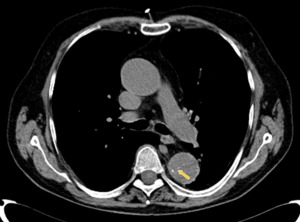
Fig. 12: Basal acquisition of CT angiography showing aortic intimal calcium displacement (yellow arrow) as a sign of aortic dissection type B of Stanford.
References: Radiology Department. Hospital Universitario La Princesa. Universidad Autónoma de Madrid (Spain)
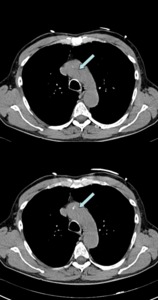
Fig. 13: A 60 year old male with chest pain and suspected AAS. Basal acquisition of CT angiography showing aortic calcium intimal flap (arrows) in a patient with aortic dissection type A of Stanford.
References: Radiology Department. Hospital Universitario La Princesa. Universidad Autónoma de Madrid (Spain)
2.
The existence of two aortic lumens (Fig.
14).
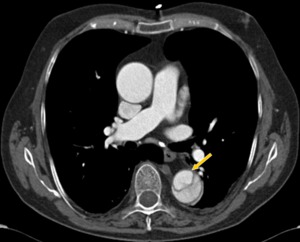
Fig. 14: CT angiography with intravenous contrast. Classic aortic dissection type B, with intimal flap and presence of two aortic lumens. The true lumen is smaller and has more density contrast (yellow arrow).
References: Radiology Department. Hospital Universitario La Princesa. Universidad Autónoma de Madrid (Spain)
The initial tear or intima-media gateway is located in areas with higher stress: ascending aorta above the aortic valve,
aortic isthmus immediately after the left subclavian artery,
the aortic arch and the abdominal aorta.
The predisposing factors are hypertension in 70% of cases,
Marfan syndrome presenting cystic medial necrosis,
bicuspid aortic valve,
iatrogeny,
and coarctation of the aorta.
In normotensive patients,
assess the possibility of cocaine intake.
Among the clinical aspects,
these patients have aortic pain: acute intense chest pain (stabbing,
tearing) also pulsatile and migrant.
It may radiate to the neck,
throat and jaw indicating ascending aorta dissection,
while if the pain is located in the abdomen or back,
the dissection is in descending aorta.
Patients present in many cases hypotension,
signs of tamponade,
decrease or asymmetry of pulses.
Other associated symptoms are stroke,
peripheral neuropathy,
syncope,
heart failure,
acute ischaemia of the upper / lower extremities,
superior vena cava syndrome,
dysphagia,
hoarseness,
haemoptysis or haematemesis.
For classification of dissections, it is used the Stanford classification suggested by Daily et al.
in 1970,
most currently accepted as being more practical than DeBakey.
It takes into account only the possible involvement of the ascending aorta and differentiates into two types:
• Type A: Includes all dissections involving the ascending aorta,
regardless of extension.
Corresponds DeBakey types I and II (Fig.
15).
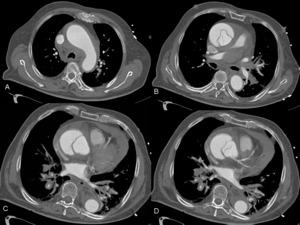
Fig. 15: A 82 year old male with chest pain and hypotension. The aortic CT angiography shows hemomediastinum and hemopericardium. It identifies intimal flap image with the same density contrast true and false lumens. He appreciates the ostium of the left coronary artery in the true lumen (image D)
References: Radiology Department. Hospital Universitario La Princesa. Universidad Autónoma de Madrid (Spain)
• Type B: Includes dissections not affecting the ascending aorta.
It corresponds to the DeBakey type III (Fig.
16).
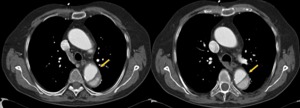
Fig. 16: Aortic CT angiography with intravenous contrast showing Stanford type B dissection with true lumen above most densely contrast (arrow).
References: Radiology Department. Hospital Universitario La Princesa. Universidad Autónoma de Madrid (Spain)
Imaging diagnosis
The two most important aspects of the diagnosis are the confirmation of dissection and the distinction between types A and B of Stanford.
Chest radiography may show indirect signs. If it is normal,
not exclude the diagnosis of dissection (Fig.
17).
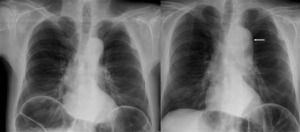
Fig. 17: A 55 year old male with abdominal pain without leukocytosis. In chest radiograph, aortic elongation is identified (left image). Twelve hours later, the patient have high intensity chest pain. The new x-ray it shows indirect signs of aortic pathology as mediastinal widening, double aortic knob contour (arrow) and tracheal deviation (right image) In Figure 21, the diagnosis of dissection type B was confirmed in CT angiography.
References: Radiology Department. Hospital Universitario La Princesa. Universidad Autónoma de Madrid (Spain)
For this diagnosis,
we need rapid diagnostic techniques and able to provide accurate information on the morphological and hemodynamic dissection: TEE (transesophageal echocardiogram),
CT (computed tomography) and MRI (magnetic resonance imaging).
The diagnostic accuracy for dissection of TEE,
CT and MRI is similar.
The CT angiography is the technique of choice,
allowing the complete study of the aorta.
We must assess:
1.
The flap dissection.
2.
Detection of both aortic lumens.
3.
Refer the entry door and relationship with coronary ostium and aortic
valve plane (Fig.
18).
4.
Presence of mediastinal haematoma,
pleural or pericardial effusion or extravasation of contrast as a sign of rupture.
5. Assessment of iliac vessels,
brachiocephalic and visceral branches relating to the true and false lumens (Fig.
19).
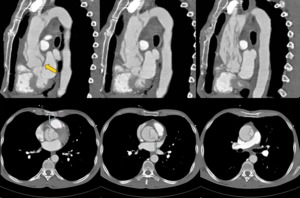
Fig. 18: A 51 year old man with acute coronary syndrome. The pain is resistant to morphine and coronary vasodilators, without clear enzyme elevation. Sagittal and axial reconstructions of CT angiography show intimal flap in ascending thoracic aorta in relation to aortic dissection type A. Both coronary arteries are perfused from the true lumen (blue arrows). The flap is seen from the valve plane (yellow arrow) and highly scattered, indicating multiple gateways. Emergency surgery was performed with aortic valve and ascending aorta replacement, with patient survival.
References: Radiology Department. Hospital Universitario La Princesa. Universidad Autónoma de Madrid (Spain)
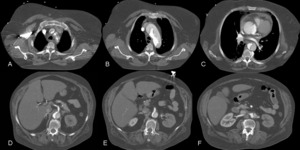
Fig. 19: Female 63 years old with clinical stroke and chest pain. It performs normal cranial CT. Suspecting aortic dissection, CT angiography was performed. It identifies Stanford type A dissection with intimal flap and double aortic lumen with different density. Involvement of supra-aortic trunks is identified (image A), hemopericardium (image C) and renal hypoperfusion (image F) by output left renal artery of the false lumen. The coronary arteries, celiac and superior mesenteric arteries are perfused by the true lumen. Bental-Bono surgery was performed. The patient survived, but with significant neurological sequelae.
References: Radiology Department. Hospital Universitario La Princesa. Universidad Autonóma de Madrid (Spain)
In our series,
we separate the two types by their different prognosis and treatment.
Dissection type A
The mean age was 62.4 years with a range between 40-87 years.
The 39% were women with a mean of 61.4 years (range 40-87 years).
The 61% were men with a mean age of 63 years (range 50-82 years).
Surgery was performed in 65% of patients with immediate postoperative mortality of 7 patients (30%).
Iatrogenic type A dissections by catheterization are diagnosed easily through iodinated contrast intramural deposit at basal chest CT (Fig.
20).
The clinical outcome is good,
except one patient in the postoperative myocardial revascularization,
died two months after nosocomial pneumonia.
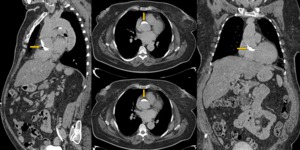
Fig. 20: Women of 63 years old with acute coronary syndrome. During coronariography, the patient presents chest pain and suggestive image of type A dissection . The diagnosis is made with the axial, sagittal and coronal reconstructions in aortic CT angiography without iodinated contrast. We observe a hyperdense crescent contrast into the aortic wall (arrows). The patient had a good clinical outcome with treatment, without progression of the dissection.
References: Radiology Department. Hospital Universitario La Princesa. Universidad Autónoma de Madrid (Spain)
Dissection Type B
It is a disease with high prevalence in male (92% of patients),
mean age 59 years old,
with range 23 to 74 years. (Fig.
21 and Fig 22).
Five patients were treated with stents (38%) and the others with conservative treatment.
In patients not treated with stents,
early mortality occurs in 30%.
One patient with mesenteric ischaemia had late mortality,
17 months after diagnosis of dissection.
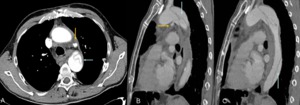
Fig. 21: A 55 year old male with high intensity chest pain. Axial and sagittal reconstructions of chest CT angiography with iodinated contrast. We can see type B aortic dissection with intimal flap image (blue arrows) and active mediastinal bleeding
(yellow arrow).
References: Radiology Department. Hospital Universitario La Princesa. Universidad Autónoma de Madrid (Spain)
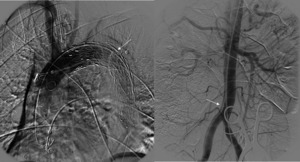
Fig. 22: A 55 years old male with with aortic dissection type B. In this patient, we can see the oclussion of the false lumen by stent in angiography (left image). In the right image, it persists intimal flap in abdominal aorta and right iliac artery (arrow).
References: Radiology Department. Hospital Universitario La Princesa. Universidad Autónoma de Madrid (Spain)
3.
Aortic intramural haematoma
It accounts for 10-30% of the AAS.
It is a variant of aortic dissection characterized by the absence of a gateway and its origin is attributed to bleeding of the vasa vasorum of the outer half of the middle layer.
It is a parietal haemorrhage and aortic flow is not detected within the aortic wall.
The diagnosis in CT angiography is a semilunar or circular thickening of the aortic wall that is denser than the lumen in the basal study.
In CT with iodinated contrast,
this spiral thickening of the aortic wall has no flow inside (Fig.
23 y 24).
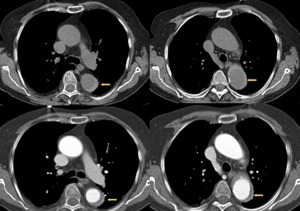
Fig. 23: A 74 years old male with chest pain and suspected AAS. In the superior images without intravenous contrast, it identifies a hyperdense crescent in descending thoracic aorta. In the images below (arrows), this thickening is not filled with contrast in relation to intramural hematoma (type B of Stanford). Conservative treatment was established.
References: Radiology Department. Hospital Universitario La Princesa. Universidad Autónoma de Madrid (Spain)
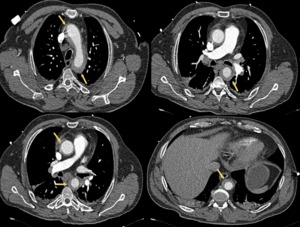
Fig. 24: A 47 year old male with chest pain. In aortic CT angiography with contrast, intramural hematoma is identified in arch and ascending thoracic aorta. Emergency surgery is performed with Bental-Bono technique with good patient outcomes. The pathological examination of the aorta confirmed bleeding and necrosis of the middle layer.
References: Radiology Department. Hospital Universitario La Princesa. Universidad Autónoma de Madrid (Spain)
The treatment is similar to classic dissection.
The type A haematoma is surgical and type B haematoma requires medical treatment.
In our series,
there were five cases of intramural haematoma: 40% female and 60% male with mean age 68.8 years,
and age range between 47 and 99 years.
In two patients underwent early surgery with Bental-Bono technique and good clinical outcome.
In the three patients,
conservative treatment was begun: one remained stable.
A second patient presented type B dissection and was treated with stents (Fig.
25 and Fig.
26).
The third patient had aortic rupture and died a month later.
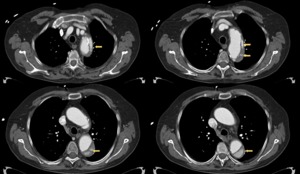
Fig. 25: A 74 year old male with chest pain and suspected AAS. In aortic CT angiography one month earlier, intramural hematoma Stanford type B is diagnosed with conservative treatment. The new study shows evolution to type B aortic dissection with intimal flap and different density of the true and false lumen. The patient was treated with stents, with good clinical outcome.
References: Radiology Department. Hospital Universitario La Princesa. Universidad Autónoma de Madrid (Spain)
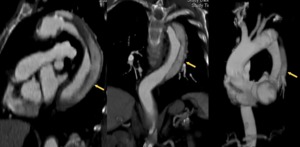
Fig. 26: A 74 years old male with chest pain and suspected AAS. In aortic CT angiography one month earlier, intramural hematoma Stanford type B is diagnosed with conservative treatment. The new study shows reconstructions sagittal, coronal and oblique with evolution to type B aortic dissection with intimal flap evidence and different density of the true and false. The patient was treated with stents, with good clinical outcome
References: Radiology Department. Hospital Universitario La Princesa. Universidad Autónoma de Madrid (Spain)
4.
Ulcerated plaques - penetrating aortic ulcer
It is an atherosclerotic lesion with ulceration of the plaque surface,
which penetrates the internal elastic lamina and allows the formation of a haematoma within the middle layer of the aorta.
Appear associated in 2.3% of patients with suspected aortic dissection and is associated with a 52% localized intramural haematoma (Fig.
27).
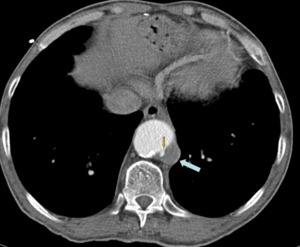
Fig. 27: A 62 years old male with chest pain that goes regularly for two years to emergency room. In aortic CT angiography, the patient had an ulcerated plaque in the descending thoracic aorta (arrows), which required treatment with stents.
References: Radiology Department. Hospital Universitario La Princesa. Universidad Autónoma de Madrid (Spain)
They are primarily located in the descending thoracic or abdominal aorta superior.
It can lead to serious complications such as saccular aneurysm,
pseudoaneurysm,
transmural rupture and dissection.
The diagnosis in aortic CT angiography can find the next signs:
1.
Eccentric accumulation of contrast within the aortic wall (Fig.
28).
2.
Thick and irregular intimal flap.
3.
Located intramural hematoma.
4.
Thickening or wall enhancement adjacent to the haematoma.
5.
Calcifications medialization
6. Draped aorta sign: The posterior margin of the aorta follows the contour and molds to adjacent vertebral body,
not identifying the posterior wall of the aorta as a definite line.
It is associated with a weak posterior aortic wall and a contained leak.
This sign represents an early stage of rupture,
when bleeding is contained by the anterior renal fascia and the dorsal root of the mesentery,
but then started to move toward the psoas muscle (Fig.
29).
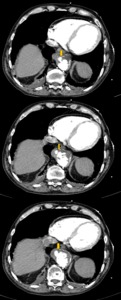
Fig. 28: A 71 years old male with suspected AAS. Aortic CT angiography images with intravenous contrast show an aortic ulcer with eccentric accumulation of contrast and mural hematoma located in the aortic wall (arrows). The patient follows up on Vascular Surgery Department, is stable and has not required surgery.
References: Radiology Department. Hospital Universitario La Princesa. Universidad Autónoma de Madrid (Spain)
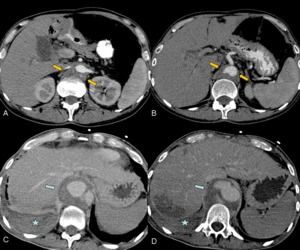
Fig. 29: A 49 year old man with epigastric pain and suspicion of AAS. Figures A and B shows the draped aorta sign (arrows). Twenty days later, the patient presented abdominal pain and hypovolemic shock. In the new aortic contrast CT angiography (Figures C and D) shows the evolution to pseudoaneurysm with signs of rupture. The patient died.
References: Radiology Department. Hospital Universitario La Princesa. Universidad Autónoma de Madrid (Spain)
The natural history is unknown and treatment should be individualized.
In our experience,
21 patients and 26 CT scans were collected,
because they are patients with multiple episodes of aortic pain.
At the CT angiography,
88% of patients are male,
with mean age of 77 years and range between 49 and 80 years.
The three female patients were mean age of 77 years and range between 68 and 86 years.
At follow-up,
only one patient died with aortic ulcer,
which develops ruptured pseudoaneurysm and died in 20 days (Fig.
30).
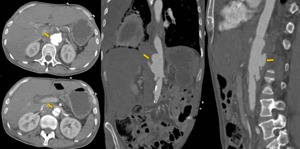
Fig. 30: A 49 years old man with epigastric pain and hypovolemic shock. The aortic contrast CT angiography with axial, coronal and sagittal reconstructions show aortic ulcer with pseudoaneurysm and signs of rupture. The patient died.
References: Radiology Department. Hospital Universitario La Princesa. Universidad Autónoma de Madrid (Spain)
Finally,
recognizing the value of CT angiography in patients without AAS according to our criteria.
In these cases,
the most common finding was aortic aneurysm (Fig.
31) and patients were referred follow-up to Vascular Surgery Department.

Fig. 31: Volumetric Reconstructions infrarenal aortic aneurysm.
References: Radiology Department. Hospital Universitario La Princesa. Universidad Autónoma de Madrid (Spain)
One patient had a deep venous thrombosis-like syndrome,
with symptoms of femoropopliteal venous thrombosis and abdominal aneurysm of nine centimeters in diameter,
not previously known.
Other diagnoses were found in the CT angiography: thrombus in the noncoronary sinus (Fig.
32),
intestinal ischaemia,
choledocholithiasis prosthetic infection (Fig.
33),
mycotic pseudoaneurysm (Fig.
34 and Fig 35),
left atrial thrombus (Fig.
36),
cardiac thrombus with multiple infarcts (Fig.
37),
lymphomatous lymphadenopathy,
pulmonary embolism,
acute cholecystitis,
gallstones in the left ureter,
aortoenteric fistulas and pulmonary neoplasia,
among others.

 and abdominal aortic aneurysm with extensive mural thrombus, with no signs of complication (image B, arrow) References: Radiology Department. Hospital Universitario La Princesa. Universidad Autónoma de Madrid (Spain)")
. References: Radiology Department. Hospital Universitario La Princesa. Universidad Autónoma de Madrid (Spain)")
, irregular posterolateral wall of the aneurysm and retroperitoneal hematoma as a sign of rupture. The patient died at surgery. References: Radiology Department. Hospital Universitario La Princesa. Universidad Autónoma de Madrid (Spain)")
 with irregular calcifications in the left wall of the aneurysm, in connection with break. Emergency surgery was performed with aortoiliac bypass and the patient continues with revisions in vascular surgery department. References: Radiology Department. Hospital Universitario La Princesa. Universidad Autónoma de Madrid (Spain)")
")
 showing aneurysm of 10 cm with hyperdense mural thrombus (yellow arrows). In the right image on CT angiography, intratrombus contrast is identified as a sign of imminent rupture(blue arrow). References: Radiology Department. Hospital Universitario La Princesa. Universidad Autónoma de Madrid (Spain)")
 and left hemothorax, in relation to aneurysm rupture. The patient died at surgery. References: Radiology Department. Hospital Universitario La Princesa. Universidad Autónoma de Madrid (Spain)")
 with extensive retroperitoneal hematoma (star). Surgery is dismissed and the patient dies. References: Radiology Department. Hospital Universitario La Princesa. Universidad Autónoma de Madrid (Spain)")
 and presence of contrast extravasation (yellow arrows). Emergency surgery is performed with an aortoiliac graft. The patient continues to make revisions at Vascular Surgery Department. References: Radiology Department. Hospital Universitario La Princesa. Universidad Autónoma de Madrid (Spain)")
. Aortoiliac graft is done urgently, with a fatal outcome. References: Radiology Department. Hospital Universitario La Princesa. Universidad Autónoma de Madrid (Spain)")
")
 as a sign of aortic dissection type B of Stanford. References: Radiology Department. Hospital Universitario La Princesa. Universidad Autónoma de Madrid (Spain)")
 in a patient with aortic dissection type A of Stanford. References: Radiology Department. Hospital Universitario La Princesa. Universidad Autónoma de Madrid (Spain)")
. References: Radiology Department. Hospital Universitario La Princesa. Universidad Autónoma de Madrid (Spain)")
 References: Radiology Department. Hospital Universitario La Princesa. Universidad Autónoma de Madrid (Spain)")
. References: Radiology Department. Hospital Universitario La Princesa. Universidad Autónoma de Madrid (Spain)")
. Twelve hours later, the patient have high intensity chest pain. The new x-ray it shows indirect signs of aortic pathology as mediastinal widening, double aortic knob contour (arrow) and tracheal deviation (right image) In Figure 21, the diagnosis of dissection type B was confirmed in CT angiography. References: Radiology Department. Hospital Universitario La Princesa. Universidad Autónoma de Madrid (Spain)")
. The flap is seen from the valve plane (yellow arrow) and highly scattered, indicating multiple gateways. Emergency surgery was performed with aortic valve and ascending aorta replacement, with patient survival. References: Radiology Department. Hospital Universitario La Princesa. Universidad Autónoma de Madrid (Spain)")
, hemopericardium (image C) and renal hypoperfusion (image F) by output left renal artery of the false lumen. The coronary arteries, celiac and superior mesenteric arteries are perfused by the true lumen. Bental-Bono surgery was performed. The patient survived, but with significant neurological sequelae. References: Radiology Department. Hospital Universitario La Princesa. Universidad Autonóma de Madrid (Spain)")
. The patient had a good clinical outcome with treatment, without progression of the dissection. References: Radiology Department. Hospital Universitario La Princesa. Universidad Autónoma de Madrid (Spain)")
 and active mediastinal bleeding
(yellow arrow). References: Radiology Department. Hospital Universitario La Princesa. Universidad Autónoma de Madrid (Spain)")
. In the right image, it persists intimal flap in abdominal aorta and right iliac artery (arrow). References: Radiology Department. Hospital Universitario La Princesa. Universidad Autónoma de Madrid (Spain)")
, this thickening is not filled with contrast in relation to intramural hematoma (type B of Stanford). Conservative treatment was established. References: Radiology Department. Hospital Universitario La Princesa. Universidad Autónoma de Madrid (Spain)")
")
")
")
, which required treatment with stents. References: Radiology Department. Hospital Universitario La Princesa. Universidad Autónoma de Madrid (Spain)")
. The patient follows up on Vascular Surgery Department, is stable and has not required surgery. References: Radiology Department. Hospital Universitario La Princesa. Universidad Autónoma de Madrid (Spain)")
. Twenty days later, the patient presented abdominal pain and hypovolemic shock. In the new aortic contrast CT angiography (Figures C and D) shows the evolution to pseudoaneurysm with signs of rupture. The patient died. References: Radiology Department. Hospital Universitario La Princesa. Universidad Autónoma de Madrid (Spain)")
")
")
. The surgery was needed for removal.
References: Radiology Department. Hospital Universitario La Princesa. Universidad Autónoma de Madrid (Spain)")
")
")
 with periaortic high density suggesting contained rupture of mycotic pseudoaneurysm, which was confirmed at surgery. References: Radiology Department. Hospital Universitario La Princesa. Universidad Autónoma de Madrid (Spain)")
, splenic infarction and thrombus in superior mesenteric artery (not shown). References: Radiology Department. Hospital Universitario La Princesa. Universidad Autónoma de Madrid (Spain)")
 References: Radiology Department. Hospital Universitario La Princesa. Universidad Autónoma de Madrid (Spain)")