ECR 2013 / C-1142
Three-dimensional MDCT evaluation in patients after partial nephrectomy: prevalence of early post-operative renal artery pseudoaneurysms
Congress:
ECR 2013
Poster Number:
C-1142
Type:
Scientific Exhibit
Keywords:
Trauma, Haemorrhage, Aneurysms, Embolisation, Computer Applications-Virtual imaging, Computer Applications-3D, CT-Angiography, CT, Catheter arteriography, Kidney, Interventional vascular, Abdomen
Authors:
T. Tajima1, M. Kohno1, T. Kondo2, S. Morita1, K. Tanabe2, S. Sakai1; 1Shinjuku-ku, Tokyo/JP, 2Shinuku-ku, Tokyo/JP
DOI:
10.1594/ecr2013/C-1142

Table 1

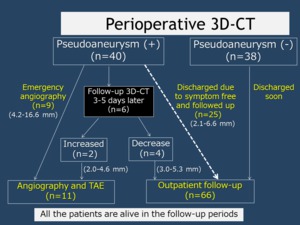
Fig. 1:
Diagram of post-operative course in patients after partial nephrectomy
. Perioperative 3D-CT 4 days after OPN demonstrated two RAPs.
C, Coronal MPR image shows one RAP in the upper pole near the surgical stump (red arrow). Another RAP located at the more proximal portion can be barely detected (blue arrow).")
Fig. 4:
Case 1. 26-year-old female with renal cell carcinoma with mild anemia...
. Perioperative 3D-CT 4 days after OPN demonstrated two RAPs.
H. Angiography after the embolization shows complete disappearance of the two RAPs. Note the microcoils located at the upper polar branch (arrows).")
Fig. 9:
Case 1. 26-year-old female with renal cell carcinoma with mild anemia...
. Perioperative 3D-CT 4 days after OPN demonstrated two RAPs.
G. Angiography was performed on the 7th post-operative day. Superselective renal arteriogram shows that a 9-mm saccular RAP at the proximal portion increased in size and protruded to the surgical stump (blue arrow). Another fusiform aneurysm was stable in size. Transcatheter arterial embolization was performed using three microcoils and gelatin sponge particles (red arrow).")
Fig. 8:
Case 1. 26-year-old female with renal cell carcinoma with mild anemia...
. Perioperative 3D-CT 4 days after OPN demonstrated two RAPs.
F. Coronal MPR image from the 3D-CT performed 2 days after A-C (Figs. 2-4) shows two RAPs in the upper pole near the surgical stump (red and blue arrows).")
Fig. 7:
Case 1. 26-year-old female with renal cell carcinoma with mild anemia...
. Perioperative 3D-CT 4 days after OPN demonstrated two RAPs.
E, Axial CT image with 1-mm thickness performed 2 days after A-C (Figs. 2-4) clearly demonstrated increase in the RAP (from 4.6 mm to 7.0 mm),")
Fig. 6:
Case 1. 26-year-old female with renal cell carcinoma with mild anemia...
. Perioperative 3D-CT 4 days after OPN demonstrated two RAPs.
D, Axial CT image with 5-mm thickness performed 2 days after A-C (Figs. 2-4) can clearly shows a RAP protruding to the surgical (arrow).")
Fig. 5:
Case 1. 26-year-old female with renal cell carcinoma with mild anemia...
.")
Fig. 10:
Case 2. 43-year-old male with renal cell carcinoma with macrohematuria....
 phase axial CT images of 5-mm thickness shows a 4-mm isodense structure in the renal hilum (arrow).")
Fig. 11:
Case 2. 43-year-old male with renal cell carcinoma with macrohematuria....
.")
Fig. 12:
Case 2. 43-year-old male with renal cell carcinoma with macrohematuria....
.
C, Renal arteriogram. Angiography was immediately performed. The RAP was visualized at the surgical stump (arrows), which was connected to the enlarged renal vein, indicating a large arteriovenous fistula (AVF). Transcatheter arterial embolization was performed using microcoils (13 Interlock-18 Fibered interlocking detachable coils (IDCs) and 3 Guglielmi detachable coils (GDCs)). A mixture of iodized oil and NBCA was additionally used to occlude the collateral pathway to the AVF.")
Fig. 18:
Case 3. 55-year-old male with renal cell carcinoma with macrohematuria and mild...
.
A, Oblique axial MPR image from the perioperative 3D-CT performed 7 days after LPN demonstrated a 10-mm bilobulated RAP near the surgical stump (arrows).")
Fig. 16:
Case 3. 55-year-old male with renal cell carcinoma with macrohematuria and mild...
.
B, Additional VR image clearly shows the early venous return (arrow).")
Fig. 17:
Case 3. 55-year-old male with renal cell carcinoma with macrohematuria and mild...
.
D, Renal arteriogram immediately after embolization. Both the RAP and the AVF were completely occluded. Note the embolic materials (arrows).")
Fig. 19:
Case 3. 55-year-old male with renal cell carcinoma with macrohematuria and mild...
.")
Fig. 14:
Case 2. 43-year-old male with renal cell carcinoma with macrohematuria....
. Perioperative 3D-CT 4 days after OPN demonstrated two RAPs.
B, Axial CT image with 1-mm thickness clearly shows a RAP protruding to the surgical defect (arrow).")
Fig. 3:
Case 1. 26-year-old female with renal cell carcinoma with mild anemia...
. Perioperative 3D-CT 4 days after OPN demonstrated two RAPs.
A, Axial CT image with 5-mm thickness shows a ill-defined hyperdense structure near the surgical stump (arrow), which cannot be recognized as a RAP.")
Fig. 2:
Case 1. 26-year-old female with renal cell carcinoma with mild anemia...
.")
Fig. 15:
Case 2. 43-year-old male with renal cell carcinoma with macrohematuria....
.")
Fig. 13:
Case 2. 43-year-old male with renal cell carcinoma with macrohematuria....