1.
Subjects
From March 27,
2012 to November 30,
2012,
the consecutive 78 patients (age,
26-82 years old; an average of 56.6 ± 11.9 years old; 56 men and 22 women) underwent 3D-CT in their perioperative periods to exclude the vascular complications after partial nephrectomy under either laparotomy (43 cases) or laparoscopy (35 cases).
The 3D-CT examinations were performed within one week after an operation (1-8 days,
an average of 4.1 days).
The tumors were located in the right kidney (n = 40) and left (n = 38): upper pole (n = 24),
central part (n = 26) or lower pole (n = 28).
The mean diameter of tumor was 3.10 ± 1.69 cm (range,
1.0-9.0 cm).
Pathologically,
there were 69 malignant and 9 benign tumors among the 78 resected tumors.
The detail of histopathological diagnoses was shown in Table 1 .
Table 1.
Results of histopathological diagnoses of the resected tumors
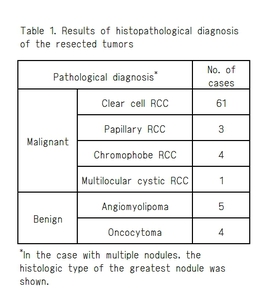
Table 1
2.
CT Technique
For dynamic CT used for perioperative 3D-CT,
helical CT imaging using a 64-row MDCT scanner was performed in a craniocaudal direction during one-breath-hold helical acquisitions using the following parameters: collimation,
0.5 mm; and CT pitch,
0.8281.
Equal amounts of each nonionic contrast agent per unit of body weight,
500-600 mgI/kg,
were used.
The injection rate was 2.5-5 mL/sec.
Bolus tracking was performed 25-30 sec after the start of injection.
The arterial phase scan was started 10 sec after the triggering level of the abdominal aorta reached +100 HU.
3.
Methods of follow-up
Ambulant follow-up was performed three weeks later after discharge,
and thereafter each three months.
Follow-up was performed in outpatient department for more than three months after surgery in all cases.
The patients underwent physical examination,
blood count,
biochemical test,
and urinalysis in outpatient department of urology.
At three weeks after a discharge,
the patients underwent follow-up contrast-enhanced CT with 5 mm-slice thickness to check up the recurrence and vascular complication.
4.
Image Processing and Data Analysis
Data were reformatted into 3D images including MPR and 50-mm slab thickness MIP using the online workstations.
Two experienced abdominal radiologists,
who had no knowledge of surgical or clinical results,
reviewed separately axial images (1-mm and 5-mm),
0.5-mm MPR image and 50-mm MIP images and assessed the numbers of early vascular complications such as a RAP,
irregularity of renal arteries and contrast extravasation.
RAP was defined as the localized dilatation of the renal artery branch whose outer diameter is 1.5 times larger as compared with the proximal portion of the lesion.
When the dilatation of the renal artery branch occurred at the stump of the renal artery branch,
a lesion larger than 2 mm was defined a significant aneurysm.
The longer axis of RAP was measured twice,
and the mean diameter of RAP was calculated.
The disagreement of interpretation was solved by consensus.
The detection rate of each reconstruction method was calculated on the basis of the highest detection rate among the four reconstruction methods.
5.
Evaluation
We performed a retrospective analysis of the 78 patients as follows:
1.
The prevalence of the early vascular complications (RAP,
extravasation,
and irregularity of renal arterial branch) in perioperative 3D-CT (1-mm axial image).
2.
The difference in detection rate of the early vascular complications among the reconstruction methods (1-mm or 5-mm axial image,
0.5-mm MPR image and 50-mm MIP image).
3.
Natural history of the RAP in cases that a RAP was followed up using 3D-CT.


