The following 3 illustrative cases of neuroblastoma as a cause of pediatric Horner Syndrome were 2 boys and 1 girl,
of about 7 to 8 months of age .
Two of them were studied with X-ray,
CT,
MRI and bone/MIBG scans,
the third one did not get any CT imaging.
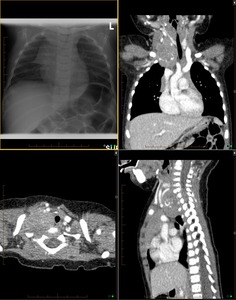
Fig. 2: 7 month old boy with intermittent right side Horner Syndrome. Anterioposterior radiograph of the chest shows left devation of the trachea from a right upper hemithorax dense opacity. Multiplanar CT shows a partially calcified solid mass lesion located at the rigth inlet of the chest with evidence of intraspinal extension and mass efect on the adjacent trachea and right sided cervical vessels.
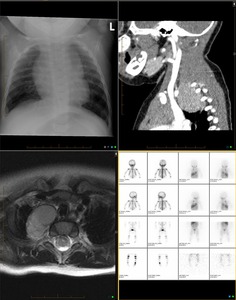
Fig. 3: 8 months old boy with right side Horner Syndrome. Anteroposterior chest X-ray shows minimal irregularity in the superior aspect of the right mediastinal contour. Saggital CT demonstrates a homogeneus solid lesion of the R apex, extending to the posterior mediastinum in the right paravertebral space. Axial T2 MR shows again a right superior and posterior mediastinal mass without evidences of intraspinal extension.MIBG scan of the same patient displays a small area of increased uptake in the right upper chest in paraspinal region.
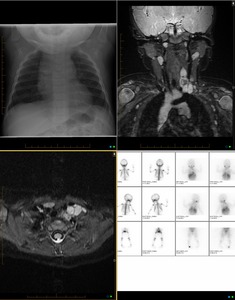
Fig. 4: 8 months old girl, left Horner Syndrome. Anteroposterior chest X-ray shows no gross abnormalities. Coronal and axial STIR MRI detect a left sided paraspinal multilobulated mass lesion, located at the base of the neck, mostly hyperintense with a relative central area of hypointensity which may be related to calcification. This lesion displaces the trachea to the right side as well as the carotid artery and jugular vein anteriorly. MIBG scans show a corresponding area of increased uptake in the left neck base.
Discussion
Based on anatomic and physiopathology background,
we recommend the physician involved in inital clinical assessment of APHS to first request a Chest Xray (CXR) with frontal and lateral projections, thus at the time of the primary assessment,
to look for any mediastinal or apical chest mass lesion.
A positive CXR will help to adapt the coverage of further cross-section imaging.
A negative CXR does not preclude for a small or centrally located mass lesion.
The second step of imaging will be best done by MRI of the head,
neck and upper chest,
with the field of view extending from the cavernous sinuses to the mid-thoracic spine including T2-T3 vertebrae. Fat saturated Spin Echo T2-weighted sequences in coronal and axial planes,
in addition to T1-weighted sequences without and with fat saturation,
latest done without and with contrast are best assessing the regions of interest.
If technical information of post-ganglionic origin of the Horner's syndrome is supected,
Time of flight angiogram (TOF-MRA) of the neck vessels should be added.
Enhanced CT of the head,
neck and upper chest could represent an alternative; however,
limitations are due to radiation dose delivered tosenstive organs,
in addition to beam hardening artifacts known to compromise the quality of images at the posterior fossa and thoracic inlet levels.
CT remains a faster and more available technique of imaging compared to MRI. CT is mostly indicated if traumatic injury of the skull base is suspected to be the cause of APHS.
Role of ultrasound of the neck is very limited if not none.
Regardless its result,
further cross-section imaging will be needed to cover the US-blinded regions as well as to better define the extent of the anomaly is any.
Role of MIBG is out of initial radiological approach; however it is an interesting technique to characterize the nature of a posterior neck or apical chest mass in pediatric population when neuroblastoma is suspected.
As well it can help screening for other lesions of similar nature.
