ECR 2013 / C-1479
Variants and vascular anomalies of supra-aortic trunks and circle of Willis: A Pictorial Review.
Congress:
ECR 2013
Poster Number:
C-1479
Type:
Educational Exhibit
Keywords:
Computer Applications-Detection, diagnosis, CT-Angiography, Catheter arteriography, Neuroradiology brain, Anatomy, Congenital
Authors:
M. M. Padilla Deza1, D. Rodriguez2, L. Aja Rodriguez3, P. Mora Montoya3, Y. P. Velasco Díaz4, A. Muntané Sánchez4; 1Hospitalet de Llobregat, Ba/ES, 2El Vendrell/ES, 3Barcelona/ES, 4Hospitalet de Llobregat /ES
DOI:
10.1594/ecr2013/C-1479

Fig. 1:
Common brachiocephalic trunk: Both common carotid arteries and the right...

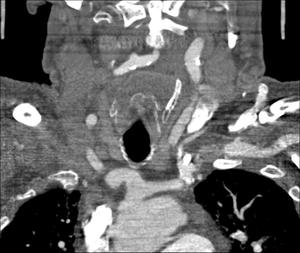
Fig. 2:
Aberrant Right Subclavian Artery: It courses to the right behind the esophagus...

Fig. 3:
Variations in the sequence of branching

Fig. 4:
• Common trunk for both carotids.

Fig. 5:
Hypoplasia of the Internal carotid Artery

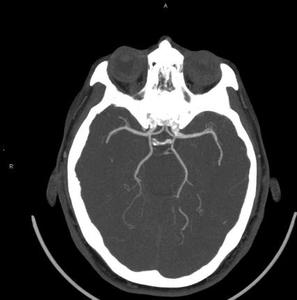
Fig. 6:
Hypoglosal artery:
A.Angio-CT, axial view.
B.VR reconstruction.
. B(left)")
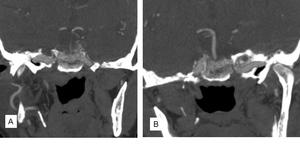
Fig. 8:
Aberrant internal carotid artery.A(right). B(left)

Fig. 7:
Hypoglosal artery. Sagital view

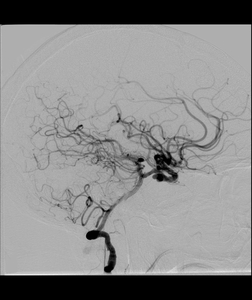
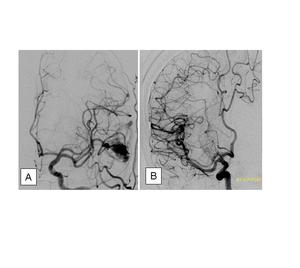
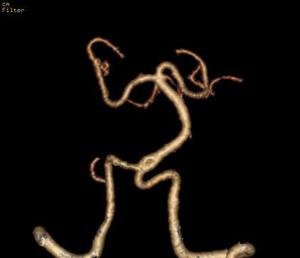
Fig. 9:
DSA. Persistent trigeminal artery

Fig. 10:
DSA. Persistent trigeminal artery

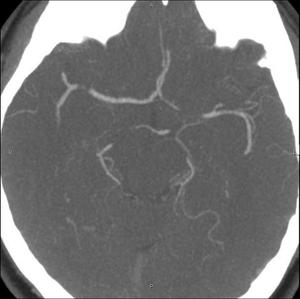
Fig. 11:
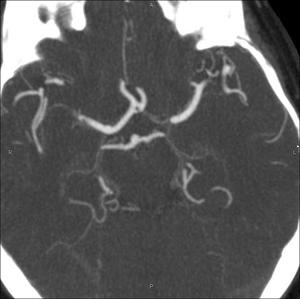
Fenestration of the anterior cerebral artery

Fig. 12:
Fenestration of the comunicante anterior artery and hypoplasia A1.

Fig. 13:
Hypoplasia A1

Fig. 14:
cerebral media accesory

Fig. 15:
MCA.
A. Duplication
B. Accesory

Fig. 16:
Hypoplasia P1

Fig. 17:
Fenestration of the basilar artery