Central nervous system (CNS) TB
CNS TB can affect the meninges,
brain or spinal cord.
This usually occurs secondary to haematogenous spread,
which can cause meningitis,
tuberculomas,
abscesses,
cerebritis or miliary TB.
TB Meningitis
Imaging findings suggestive of TB meningitis include homogenous meningeal enhancement,
which occurs usually in the basal cisterns and can extend into the interhemispheric fissures and around the spinal cord (Fig.
2).
TB meningitis can result in hydrocephalus and infarcts in a middle cerebral artery distribution due to arteritis of the vessels within the basal cisterns[3].
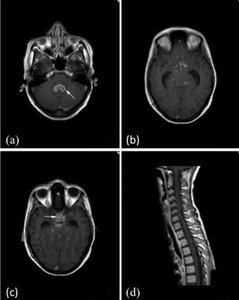
Fig. 2: T1 post gadolinium imaging of a 26 year old female patient with a 3 week history of meningism and cranial nerve palsies following a trip to India. Figure (a) shows thick ependymal enhancement within the fourth ventricle in keeping with ependymitis secondary to TB. Figures (b) and (c)show classical nodular leptomeningeal enhancement within the basal cisterns commonly seen with TB, which extends into the pituitary fossa (arrow). Prominent temporal horns of the lateral ventricles indicate early hydrocephalus. (d) is a sagittal section through the cervical and upper thoracic spine showing extension of the intracranial TB leptomeningeal meningitis around the spinal cord.
Tuberculomas
Tuberculomas can be solitary or multiple and are usually found in the frontal or parietal lobes.
On CT they appear as round,
lobulated,
homogenous ring enhancing lesions with irregular wall thickness.
On MRI those tuberculomas that are non-caseating are hyperintense on T2WI with homogenous enhancement whereas caseating lesions are iso to hypointense on T2WI with rim enhancement[2] (Fig.
3).
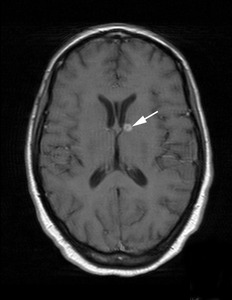
Fig. 3: Axial T1 post gadolinium MRI of a 37 year old patient with known HIV and TB. The image shows a ring enhancing lesion adjacent to the frontal horn of the left lateral ventricle consistent with a tuberculoma. A similar lesion was also seen in the left temporal lobe.
Disease mimics include infections such as toxoplasmosis and fungal infections,
malignancy such as lymphoma,
metastases and primary brain tumors and other granulomatous disease such as sarcoidosis.
Musculoskeletal TB
Spondylitis
Spondylitis (or Pott Disease) is the most common musculoskeletal presentation of TB.
It most commonly involves the thoracolumbar region and preferentially affects the vertebral body to the posterior elements.
There is slow progression of infection with relative preservation of the intervertebral disc height and lack of sclerosis.
Later in the infective process,
the patient may develop anterior wedging of the affected vertebral body resulting in a focal kyphosis (gibbus deformity).
Often more than one level is affected with spread of infection resulting from direct extension into the adjacent disc or subligamentous spread beneath the longitudinal ligaments to adjacent vertebral bodies. Disease extension to the intervertebral discs and adjacent soft tissue usually occurs anterolateral to the vertebral body and is often seen as paravertebral abscesses and psoas abscesses (Fig.
4).
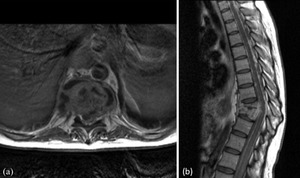
Fig. 4: MRI images from a 26 year old male with known TB meningitis presenting with back pain and urinary retention. (a) is an axial T1 post gadolinium image through T9 showing an anterolatereal paraspinal mass with irregular enhancement, typical features of a TB paraspinal abscess. (b) is a sagittal T1 post gadolinium image showing T9/T10 spondylodiscitis with wedge compression of T9 and T10 resulting in kyphosis. Also, note the nodular meningeal enhancement throughout the thoracic spine.
If extension is extensive,
erosion of neighbouring structures can occur,
as in figure 5,
where erosion of the posterior oesophagus has occurred due to adjacent spondylitis.
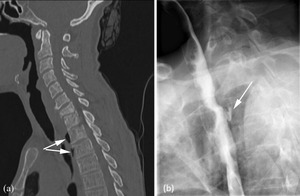
Fig. 5: Images of a 43 year old female with confirmed TB lymphadenitis and cervical spondylitis. (a) is a sagittal CT through the cervical and upper thoracic spine showing destruction of the C7 and T1 endplates with anterior loss of height of C7 in keeping with TB spondylitis. The arrows point to a collection of gas anterior to T2 and T3 secondary to oesophageal perforation. (b) is a barium swallow showing the localised posterior oeosphageal leak at T3 (arrow) as a result of the adjacent osteomyelitis.
CT is good for identifying small foci of vertebral involvement whereas MRI is useful for looking at intervertebral disc involvement,
which is usually seen as low T1 signal and high T2 signal within the discs and to detect subtle bone marrow changes in adjacent vertebrae that may be missed on CT (Fig.
6).

Fig. 6: Multifocal TB spondylitis and extensive paraspinal abscesses in a 29 year old with a 2 year history of back pain, weight loss and night sweats. Images show patchy high T2 signal in multiple vertebral bodies (a) which show corresponding low signal on T1WI (b) and abnormal enhancement post gadolinuium (c). In addition there are extensive, enhancing, anterior paraspinal collections throughout the spine (a, b and c).
Disease mimics include other pyogenic infections and metastatic disease.
Findings suggestive of TB include: calcification of paravertebral abscess and relative preservation of the intervertebral disc[2].
TB Osteomyelitis
TB osteomyelitis is usually due to haematogenous spread and typically affects the metaphysis.
Imaging findings are similar to those of osteomyelitis from other causes (Fig.
7).
Features that help distinguish TB osteomyelitis from pyogenic causes are the presence of transphyseal spread and the presence of imaging findings of osteomyelitis at the time of presentation rather than 2-3 weeks later,
as typically seen in pyogenic infections.
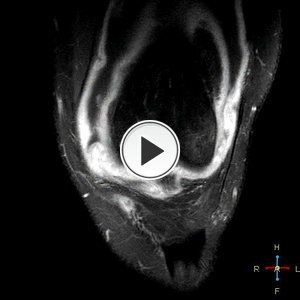
Fig. 7: T1 fat sat post contrast coronal images of the left knee. Osteomyelitis with septic arthritis and intra osseous abscess formation. Contrast enhancing collection within the posterolateral aspect of the lateral femoral condyle and extensive surrounding oedema present. There is considerable synovial enhancement throughout the knee joint.
TB arthritis
TB arthritis can result from either haematogenous spread or direct spread from an area of osteomyelitis and typically occurs in large,
weight-bearing joints such as the hip and knee.
(Fig 8).
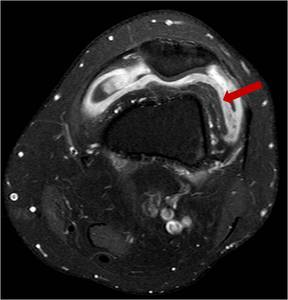
Fig. 8: Axial T1 fat sat post iv contrast T2 knee showing joint effusion and enhancing thickened synovium (arrow)in the left knee. Same patient as figure 7 but post 6 weeks anti-TB treatment. TB arthritis and osteomyelitis often present in the same joint.
The plain film imaging findings are very similar to those of rheumatoid arthritis; peri-articular osteopenia,
erosions and loss of joint space.
Imaging findings to help discriminate TB from rheumatoid disease are that TB is usually monoarticular and has relative preservation of joint space until later on in the disease[3]. Imaging features to help distinguish TB from pyogenic arthritis on MRI are that TB is more likely to have bone erosions,
extra-articular extension and the abscesses seen will tend to have a thin,
smooth rim rather than a thick,
irregular rim as seen in pyogenic infections[4].
Psoas abscess
Psoas abscess commonly occur from spondylitis as described above,
however psoas abscesses can occur independently and cause local bone destruction as seen in figure 9.
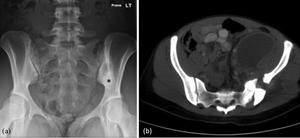
Fig. 9: 23 year old female who presented with left hip pain and night sweats who was later confirmed to have TB. Initial plain film (a) shows increased bone density adjacent to the left sacro-iliac joint (SIJ) (asterix). The patient went on to have a CT (b) which shows a large left psoas abscess tracking into the gluteus medius muscle resulting in destruction and sclerosis of the left ala and SIJ.
Lymphadenopathy
Lymphadenopathy is a common presentation of extra-pulmonary TB.
Mediastinal lymphadenopathy often occurs in association with pulmonary TB,
cervical lymphadenopathy is one of the most common extra-pulmonary presentations of TB in children and abdominal lymphadenopathy is the commonest presentation of abdominal TB in adults and will be discussed in more detail later.
TB lymphadenopathy is often seen on ultrasound as large,
round,
heterogeneous lymph nodes with necrotic centres (Fig.
10).

Fig. 10: TB lymphadenopathy. Two markedly enlarged, hypoechoic, rounded, centrally necrotic (arrow) lymph nodes within the left axilla in patient with TB.
Calcification can occur later on,
but is not usually seen at the time of presentation.
On CT,
lymphadenopathy is seen as peripherally enhancing,
enlarged lymph nodes with low-density (necrotic) centres.
Chest wall TB
The chest wall is affected in 1-5% of cases of musculoseletal TB (Fig.
11).
TB abscess of the chest wall can affect the sternum,
costochondral junction,
rib,
costovertebral joint and vertebrae.
Although metastases are the primary cause of rib destruction,
TB is the second most common cause of soft tissue mass causing bony rib destruction.
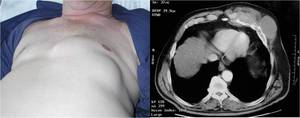
Fig. 11: Elderly patient presented with chest wall mass. Note that the mass is centred on the left anterior rib and costochondral junction with bony destruction. Biopsy proven TB. Unusually the soft tissue mass is not necrotic.
Abdominal TB
TB within the abdomen is the most common extra-pulmonary site.
The most common sites of abdominal TB in decreasing frequency are lymph nodes,
the genitourinary tract,
peritoneal disease and gastrointestinal tract[5].
Lymph nodes
Lymphadenopathy is the most common abdominal presentation of TB[5].
Abdominal lymphadenopathy occurs due to haematogenous spread,
direct spread from the gastro-intestinal tract and serosal surfaces of neighbouring organs.
The lymph nodes are often 2-3cm in size,
are of low density due to necrotic centres and have an enhancing rim.
These lymph nodes may coalesce and develop a multilocular appearance (Fig.
12). Following treatment and healing they may calcify.

Fig. 12: Multiple, confluent, peripherally enhancing centrally necrotic lymph nodes in the mesentery and right common iliac region (asterix) of a patient presenting with abdominal TB.
Peri-portal,
mesenteric and peripancreatic groups of lymph nodes are most commonly affected within the abdomen[5] (Fig.
13).
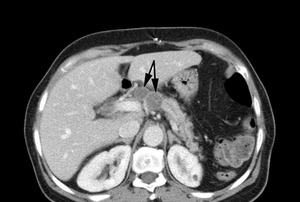
Fig. 13: Biopsy proven peri-pancreatic TB. The image shows several low density, peripherally enhancing peripancreatic nodes: a typical distribution for abdominal TB lymphadenopathy.
Although peripheral enhancement of lymph nodes is typical for TB it is also seen in other disease such as necrotic metastases,
pyogenic infections and Whipple’s disease[6].
Features to help distinguish TB from lymphoma are that lymphadenopathy caused by TB tends be less than 4cm,
have a peripheral enhancing rim and tends to preferentially affect peripancreatic and ileo-caecal regions whereas lymphoma lymphadenopathy tends to be larger than 4cm,
show homogenous enhancement and is more likely to affect the lower para-aortic region[5,
7].
Renal TB
Renal parenchyma and the upper collecting system are often affected together.
The earliest imaging findings are those of papillary necrosis,
which gives a moth eaten appearance to the calyx due to ulceration.
In addition,
there may be small focal areas of reduced enhancement in the region of the medullary pyramids and cavity formation. Later on strictures occur within the collecting system.
Depending on where these occur there can be dilatation of focal calyces or the complete collecting system (Fig.14).
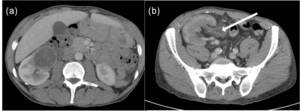
Fig. 14: (a) Patient presenting with renal mass identified on ultrasound and pulmonary TB. The low density renal abscess is an unusual presentation of a Tuberculoma.
(b) Patient with biopsy proven TB in the renal transplant in the right iliac fossa. Note the enlargement of the transplant kidney and dilatation of the collecting system and renal pelvis with abnormal urothelial enhancement.
If there are multiple strictures a beaded appearance results.
Alternatively there may be incomplete opacification of an entire calyx due to fibrosis (a phantom calyx).
Finally,
autonephrectomy can result which appears as a small,
shrunken,
scarred kidney,
often with hydronephrosis and ‘putty like calcification’ forming a cast of the kidney[8,
1].
Various types of calcification can be seen within the kidney at various stages of TB renal disease including amorphous,
granular,
curvilinear or lobar (putty) calcifications.
Renal TB can uncommonly present as a focal renal abscess (a tuberculoma) as in figure 13.
In terms of imaging,
urography is the best at detecting early uroepithelial damage,
whereas CT is better at looking at the extent of calcification and extra-renal spread.
Disease mimics include other causes of papillary necrosis,
focal bacterial nephritis,
xanthogranulomatous pyelonephritis and transitional cell carcinoma.
Ureteric TB
Appearances of ureteric TB consist of ulcers and strictures.
The latter can lead to a beaded appearance of the ureter and chronically,
a shortened/straight,
pipe-stem appearance to the ureter.
CT is good at demonstrating peri-ureteral fat stranding and thickening of the ureteral wall.
Bladder TB
Early disease is seen as mucosal ulceration and wall oedema.
Occasionally filling defects are seen due to granulomas in the wall.
Advanced disease shows a thick,
contracted bladder with reduced bladder capacity due to fibrosis.
Calcification of the bladder wall is rare and can be seen in other disease mimics such as schistosomiasis,
radiation,
carcinoma or an encrusted foreign body.
Female genital tract TB
TB salpingitis almost always presents as bilateral tubo-ovarian abscesses that extend into the extra-peritoneal cavity[2].
Typical imaging findings on hysterosalpingography suggestive of TB are obstruction of the fallopian tubes,
multiple strictures,
deformity and obliteration of endometrial tract and calcified lymph nodes[8].
The MR appearances of TB salpingitis are shown in figure 15.
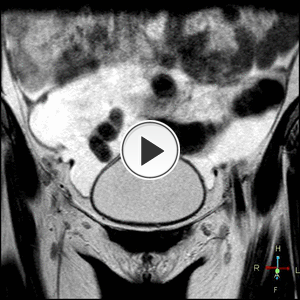
Fig. 15: Coronal T2 weighted MRI pelvis. Bilateral complex adnexal masses and dilated fluid filled fallopian tubes.
Male genital tract TB
The male genital tract is also susceptible to TB infection resulting in prostate abscesses,
epididymitis and epididymo-orchitis.
Gastro-intestinal TB
Gastro-intestinal TB usually occurs through haematogenous spread,
direct contiguous spread from neighbouring structures e.g.
fallopian tubes,
or swallowing infected sputum.
The ileo-caecal region is the most commonly involved area in the gastrointestinal tract,
probably due to the large amount of lymphoid tissue there[3].
The most common imaging findings are ulceration,
mural thickening,
fibrosis and extraluminal fat stranding (Fig.
16).
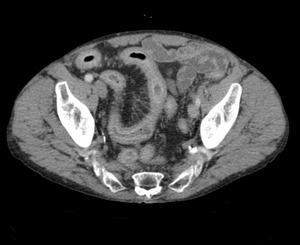
Fig. 16: Contrast enhanced CT of a patient with previously treated pulmonary TB showing a long segment of terminal ileum wall thickening with prominent mesenteric vascularity and surrounding fat stranding.
Thickening of the ileoceacal valve and/or a gaping valve with a narrowed terminal ileum is known as the inverted umbrella or Fleischner’s sign. Thickening around the ileocaecal valve can engulf it making it difficult to identify.
Fibrosis can result in annular stenoses in one or more areas,
which can lead to obstruction.
Amputation and retraction of the caecum can also occur due to fibrosis[2].
Barium studies can demonstrate ulcers,
fistulas,
an increased transit time with hypersegmentation and flocculation,
thickened folds and dilated segments or strictures.
CT and MRI are good at showing wall thickening,
enhancing mucosa,
strictures,
surrounding inflammation,
enlarged lymph nodes and any peritoneal disease (Fig.
17).
However,
small ulcers are difficult to visualise on CT and MRI.
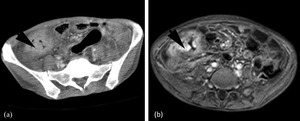
Fig. 17: 34 year old with proven abdominal TB. (a) is a contrast enhanced CT showing extensive wall thickening and mucosal enhancement of the caecum. (b) is a T1 post gadolinium MRI at the same level, again showing wall thickening and mucosal enhancement. The caecal wall thickening is so extensive the terminal ileum could not be identified.
Disease mimics include Crohn’s disease,
lymphoma and carcinoma.
Distinguishing features of TB are large,
oval ulcers (small round ulcers are seen in Crohn’s disease),
an asymmetrically thickened ileocaecal valve,
massive adenopathy and preferential thickening of the medial caecal wall[2,
6].
Peritoneal TB
Peritoneal TB is rare and is usually associated with other forms of abdominal TB.
Three types exist: wet,
fibrotic-fixed and dry.
Wet peritoneal TB consists of large amounts of viscous ascites that may be of high attenuation on CT and may be loculated.
Fibrotic-fixed peritoneal TB consists of omental masses/cake,
matted loops of bowel and mesentery and small amounts of ascites (Figs.
18 and 19).
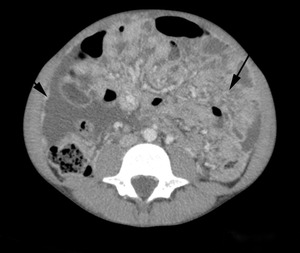
Fig. 18: Fibrotic-fixed TB in an 11 year old. The contrast enhanced CT shows nodular enhancement of the omentum (long arrow) resulting in extensive omental cake and nodular peritoneal enhancement (arrow head). A moderate amount of ascites is also seen.

Fig. 19: Coronal post contrast CT in the same child as Fig. 17 demonstrates the extent of the peritoneal disease. The child presented with weight loss, malaise and increased abdominal girth due to large volume ascites which was initially suspected to be due to a malignant process.
Dry peritoneal TB is seen as caseous nodules,
a fibrous peritoneal reaction and dense adhesions.
Disease mimics include carcinomatosis,
mesothelioma and other causes for ascites.
Distinguishing features of TB include extension of inflammation outside of the peritoneal cavity[3].
It is often very difficult to distinguish TB peritoneal disease from malignancy and aspiration of any ascitic fluid should be obtained and sent for PCR[9].
Solid viscera
The liver and spleen are the most commonly affected solid viscera within the abdomen.
This usually occurs through haematogenous spread. The affected organs can demonstrate micronodular (miliary) or macronodular disease.
Micronodular disease is more common and often associated with miliary pulmonary TB.
CT shows multiple small low attenuation foci throughout the liver or spleen (Fig.
20).

Fig. 20: Miliary TB in the spleen and liver in a patient with known miliary pulmonary TB. Contrast enhanced CT shows multiple, small, round, low density foci throughout the spleen and liver(arrows)in keeping with miliary disease.
Disease mimics include sarcoidosis,
fungal infection and lymphoma.
Macronodular disease usually consists of one or more large,
low-density mass which may calcify over time (Fig.
21) on a background of organomegally.
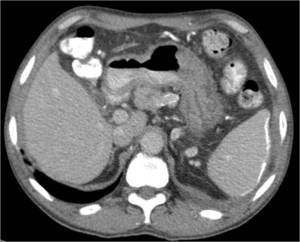
Fig. 21: Note the splenic calcification in this patient who had previous abdominal TB infection.
On MRI these tuberculomas are low signal on T1WI with a honeycomb appearance and hyperintense on T2WI with a less intense rim.
Disease mimics include primary hepatic tumors,
abscesses or metastases.
Extra-pulmonary,
Intrathoracic TB
Although pulmonary TB is the most common presentation of TB,
TB can still present within the thorax but in an extra-pulmonary location.
This includes mediastinal lymphadenopathy,
pleural disease and pericarditis.
Pleural TB
TB should always be considered in the differential diagnosis of pleural effusions especially in the setting of parenchymal abnormality (Fig.22).

Fig. 22: Chest x-ray demonstrates large left pleural effusion in a patient who subsequently had confirmed TB. Note the mediastinal and tracheal shift away from the almost-complete left whiteout. Note also the nodular opacification in the right upper lobe.
Mediastinal lymphadenopathy
As in other sites,
lympadenopathy secondary to TB infection often shows central necrosis and peripheral enhancement (Fig.23).
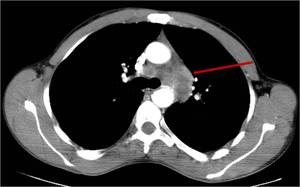
Fig. 23: Large aorto-pulmonary window mediastinal lymph nodes in a patient confirmed to have TB. Note the central necrosis and peripheral enhancement.
Pericardial TB
TB pericarditis consists of four stages: granulomas deposited in the pericardium,
pericardial effusion,
pericardial thickening (Fig.
24) and finally fibrosis and calcification resulting in constrictive pericarditis[10].
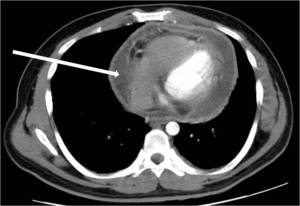
Fig. 24: Axial post iv contrast CT demonstrates large peripherally enhancing pericardial effusion (arrow). Pericardial tap diagnostic for TB.


 shows thick ependymal enhancement within the fourth ventricle in keeping with ependymitis secondary to TB. Figures (b) and (c)show classical nodular leptomeningeal enhancement within the basal cisterns commonly seen with TB, which extends into the pituitary fossa (arrow). Prominent temporal horns of the lateral ventricles indicate early hydrocephalus. (d) is a sagittal section through the cervical and upper thoracic spine showing extension of the intracranial TB leptomeningeal meningitis around the spinal cord.")

 is an axial T1 post gadolinium image through T9 showing an anterolatereal paraspinal mass with irregular enhancement, typical features of a TB paraspinal abscess. (b) is a sagittal T1 post gadolinium image showing T9/T10 spondylodiscitis with wedge compression of T9 and T10 resulting in kyphosis. Also, note the nodular meningeal enhancement throughout the thoracic spine.")
 is a sagittal CT through the cervical and upper thoracic spine showing destruction of the C7 and T1 endplates with anterior loss of height of C7 in keeping with TB spondylitis. The arrows point to a collection of gas anterior to T2 and T3 secondary to oesophageal perforation. (b) is a barium swallow showing the localised posterior oeosphageal leak at T3 (arrow) as a result of the adjacent osteomyelitis.")
 which show corresponding low signal on T1WI (b) and abnormal enhancement post gadolinuium (c). In addition there are extensive, enhancing, anterior paraspinal collections throughout the spine (a, b and c).")
in the left knee. Same patient as figure 7 but post 6 weeks anti-TB treatment. TB arthritis and osteomyelitis often present in the same joint.")
 shows increased bone density adjacent to the left sacro-iliac joint (SIJ) (asterix). The patient went on to have a CT (b) which shows a large left psoas abscess tracking into the gluteus medius muscle resulting in destruction and sclerosis of the left ala and SIJ.")
 lymph nodes within the left axilla in patient with TB.")

 of a patient presenting with abdominal TB.")

 Patient presenting with renal mass identified on ultrasound and pulmonary TB. The low density renal abscess is an unusual presentation of a Tuberculoma.
(b) Patient with biopsy proven TB in the renal transplant in the right iliac fossa. Note the enlargement of the transplant kidney and dilatation of the collecting system and renal pelvis with abnormal urothelial enhancement.")

 is a contrast enhanced CT showing extensive wall thickening and mucosal enhancement of the caecum. (b) is a T1 post gadolinium MRI at the same level, again showing wall thickening and mucosal enhancement. The caecal wall thickening is so extensive the terminal ileum could not be identified.")
 resulting in extensive omental cake and nodular peritoneal enhancement (arrow head). A moderate amount of ascites is also seen.")
in keeping with miliary disease.")



. Pericardial tap diagnostic for TB.")