ECR 2013 / C-2247

EXTRA-ARTICULAR CAUSES OF COXALGIA: Present and new concepts
Congress:
ECR 2013
Poster Number:
C-2247
Type:
Educational Exhibit
Keywords:
Musculoskeletal system, Musculoskeletal soft tissue, Musculoskeletal joint, CT, MR, Ultrasound-Power Doppler, Arthrography, Acute, Congenital, Connective tissue disorders
Authors:
V. Mascarenhas, F. Morais, P. D. Afonso, A. Guerra, H. M. R. Marques, A. M. Gaspar; Lisbon/PT
DOI:
10.1594/ecr2013/C-2247

Fig. 1:
Coronal T1 WI of the left hip. Fracture line on the inner facet of the femoral...
 surrounded by oedema (hyperintense signal). References: Hospital da Luz - MSK Imaging Unit - Lisbon/PT")
Fig. 2:
Coronal PD Fat-Sat WI of the left hip. Fracture line on the inner facet of the...

Fig. 3:
CR of the right hip. Fracture line on the sub-articular region of the femoral...

Fig. 4:
Sagital PD Fat-Sat WI of the left hip. Fracture line on the sub-articular...

Fig. 5:
Coronal PD T2 WI of the right hip. Fracture line on the sub-articular region of...
 with no fracture line seen. References: Hospital da Luz - MSK Imaging Unit - Lisbon/PT")
Fig. 6:
Coronal T2* Fat-Sat WI of the pelvis. Oedema of the head and neck of the left...

Fig. 7:
Coronal PD Fat-Sat WI of the left hip. Oedema of the head and neck of the left...

Fig. 8:
Coronal T1WI of the left hip. Oedema of the head and neck of the left femur.

Fig. 9:
Coronal T2 Fat-Sat WI of the pelvis. Evident oedema of the symphysis pubis.

Fig. 10:
Axial PD Fat-Sat WI of the pelvis. Evident oedema of the symphysis pubis.
 due to metastatic breast cancer. References: Hospital da Luz - MSK Imaging Unit - Lisbon/PT")
Fig. 11:
CR of the left hip. Pathological fracture of the left femur (arrow) due to...

Fig. 12:
Coronal PD WI of the left hip. Pathological fracture of the left femur due to...

Fig. 13:
Axial PD Fat-Sat WI of the left hip. Pathological fracture of the left femur...

Fig. 14:
Sagital CT image. Iliac bone lytic lesion due to metastatic breast cancer

Fig. 15:
Axial CT image. Multiple osteolytic lesions of multiple myeloma at the first...
 - lymphoma. References: Hospital da Luz - MSK Imaging Unit - Lisbon/PT")
Fig. 16:
Axial T2 Fat-Sat WI of the pelvis. Hyperintense soft tissue mass (arrow) -...

Fig. 17:
CR of the right hip. Femoral focal dense lesion on the inner facet of the...

Fig. 18:
Coronal CT image of the right hip. Femoral focal dense lesion on the inner...
. References: Hospital da Luz - MSK Imaging Unit - Lisbon/PT")
Fig. 19:
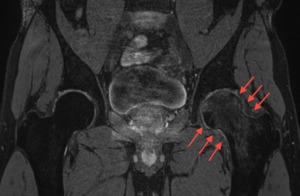
CR of the left hip. Acetabular osteolytic lesion (arrows).
. References: Hospital da Luz - MSK Imaging Unit - Lisbon/PT")
Fig. 20:
Axial CT image of the left hip. Acetabular osteolytic lesion with discrete...
. References: Hospital da Luz - MSK Imaging Unit - Lisbon/PT")
Fig. 21:
Coronal CT image of the left hip. Acetabular osteolytic lesion with discrete...
. References: Hospital da Luz - MSK Imaging Unit - Lisbon/PT")
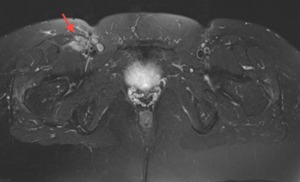
Fig. 22:
Axial T1WI of the pelvis. Right juxta-trochanteric mass with low-signal on T1...
. References: Hospital da Luz - MSK Imaging Unit - Lisbon/PT")
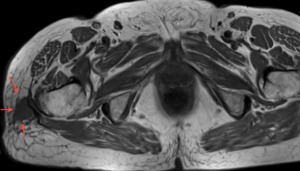
Fig. 23:
Coronal T1WI of the right hip. Mass in the right inguinal area with low signal...
. References: Hospital da Luz - MSK Imaging Unit - Lisbon/PT")
Fig. 24:
Sagital PD Fat-Sat WI of the right hip. Mass in the right inguinal area with...

Fig. 25:
Coronal T1WI of the right hip. Hematoma of the right ischio-femoral space in a...

Fig. 26:
Axial T1 Fat-Sat WI of the right hip. Hematoma of the right ischio-femoral...

Fig. 27:
Axial T1 Fat-Sat GAD WI of the right hip. Hematoma of the right ischio-femoral...

Fig. 28:
Coronal PD Fat-Sat WI of the left hip. Acute complete muscular rupture of the...
 of the left hip. Muscular rupture of the gluteus minimus (arrows) with trochanteritis. References: Hospital da Luz - MSK Imaging Unit - Lisbon/PT")
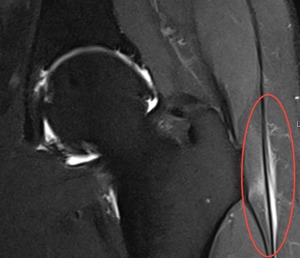
Fig. 29:
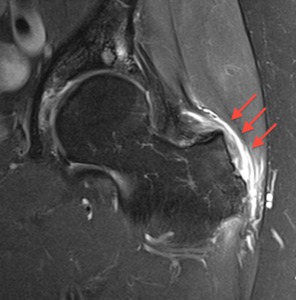
Coronal PD Fat-Sat WI (arthro- MRI) of the left hip. Muscular rupture of the...
 with surrounding oedema at the enthesis of the gluteus medius muscle with bursitis (red arrows). References: Hospital da Luz - MSK Imaging Unit - Lisbon/PT")
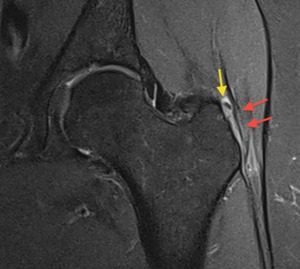
Fig. 30:
Coronal PD Fat-Sat WI of the left hip. Tiny calcification (yellow arrow) with...
. References: Hospital da Luz - MSK Imaging Unit - Lisbon/PT")
Fig. 31:
Coronal PD Fat-Sat WI of the right hip. Peri-trochanteric bursitis (arrows).

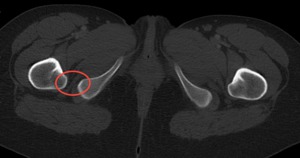
Fig. 32:
Coronal CT image of the pelvis. Bilateral narrowing between the ischium and...

Fig. 33:
Axial CT image shows bilateral narrowing between the ischium and lesser...
. References: Hospital da Luz - MSK Imaging Unit - Lisbon/PT")
Fig. 34:
3D CT reformats of the pelvis. Bilateral reduction of the space between lesser...

Fig. 35:
Axial CT image shows right narrowing between the ischium and lesser trochanter.

Fig. 36:
Coronal PD Fat Sat WI of the left hip. Diffuse thickening of the proximal left...

Fig. 37:
Sagital T2WI. Apophyseal and discal degeneration with foraminal stenosis.

Fig. 38:
Coronal T2WI. Right lumbar degenerative scoliosis.

Fig. 39:
Sagital T1WI. Exuberant disc and apophyseal joint degenerative changes with...

Fig. 40:
Axial T2WI. Exuberant disc and apophyseal joint degenerative changes with...

Fig. 41:
Sagital T2WI. Right posterior L5-S1 level spinal disc herniation, causing S1...

Fig. 42:
Sagital T2WI. Osteosclerotic L5 bone prostatic metastasis occupying most of the...

Fig. 43:
Sagital T1 Fat-Sat GAD WI. Exuberant posterior facet degeneration with synovial...

Fig. 44:
Axial CT image of the sacroiliac joints. Prominent sacroiliac subchondral...

Fig. 45:
Coronal CT image of the sacroiliac joints. Prominent sacroiliac subchondral...
. References: Hospital da Luz - MSK Imaging Unit - Lisbon/PT")
Fig. 46:
Coronal T1WI of the sacroiliac joints. T1 hypointensity of subchondral bone...
. References: Hospital da Luz - MSK Imaging Unit - Lisbon/PT")
Fig. 47:
Coronal T2 Fat-Sat WI of the sacroiliac joints. Hyperintensity of subchondral...
 - Paget disease References: Hospital da Luz - MSK Imaging Unit - Lisbon/PT")
Fig. 48:
Coronal CT image of the pelvis. Cortical thickening and trabecular coarsening...
 - Paget disease References: Hospital da Luz - MSK Imaging Unit - Lisbon/PT")
Fig. 49:
Axial CT image of the pelvis. Cortical thickening and trabecular coarsening...
 . References: Hospital da Luz - MSK Imaging Unit - Lisbon/PT")
Fig. 50:
Axial T1 Fat-Sat GAD WI of the pelvis. Septic sacroiliitis complicated by...