Benign conditions involving the salivary glands can be divided into:
- Sialolithiasis
- Non-Infectious Inflammation
- Infectious Inflammation
- Cystic Lesions
- Benign Tumours
1.Sialolithiasis
Sialolithiasis is the second most common disease of the salivary glands after mumps.
It typically presents with painful swelling of the gland.
The submandibular gland is most commonly affected accounting for 85% of all salivary gland calculi due to the high mucus content of its secretions.
Non contrast CT has the highest sensitivity for calculus detection.
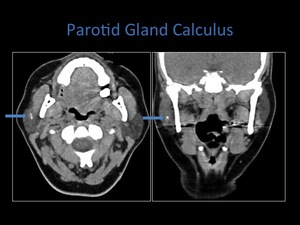
Fig. 6: Axial and coronal non contrast CT demonstrating a calculus within the right parotid gland.
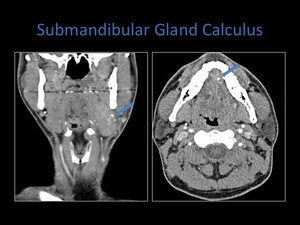
Fig. 7: Axial and coronal contrast enhanced CT demonstrating a calculus within the left submandibular gland. A contrast enhanced CT was performed as the clinical question was unclear.
Infectious Inflammation
Paramyxo and cytomegalovirus are the most common viral infections of the salivary glands.
Staph aureus is the most common bacterial infection.
Granulomatous infections also occur- tuberculosis.
If an abscess is suspected a contrast enhanced CT should be performed.
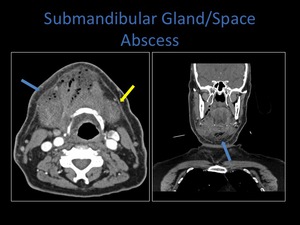
Fig. 8: Axial and coronal contrast enhanced CT demonstrating a diffuse mass containing air pockets within the submandibular space. Note the involvement of the right platysma muscle (blue arrow) and the normal left platysma muscle (yellow arrow).
Non-Infectious Inflammation
A number of autoimmune diseases involve the salivary glands including HIV,
Sjogren disease and Sarcoidosis.
Sjogren disease and sarcoidosis predispose to calculus formation.
Sjogren disease also increases the risk of parotid lymphoma.
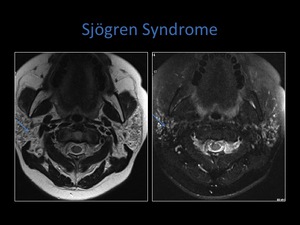
Fig. 9: Axial T1 and T2 fat sat sequences of the parotid gland. Note the salt and pepper appearance, low signal on T1 and high signal on T2 indicating tiny cystic spaces.
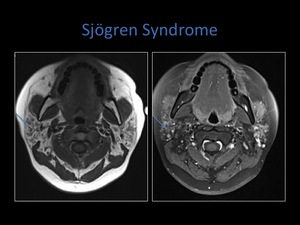
Fig. 10: Axial T1 and T1 post contrast sequences demonstrating some enhancement of the solid areas within the involved parotid gland.
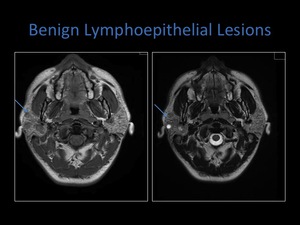
Fig. 11: Axial T1 and T2 MRI sequences demonstrating bilateral intraparotid solid and cystic masses in a patient with known HIV.
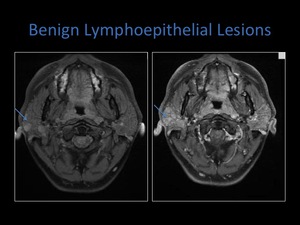
Fig. 12: Axial T1 MRI pre and post contrast demonstrating enhancement post contrast.
Cystic Lesions
Cystic lesions involving the floor of the mouth are commonly seen.
The most frequent is a ranula;which can be divided into simple and diving.
A ranula is a mucous retention cyst with an epithelial lining which arises from the sublingual glands or minor salivary glands.
A simple ranula lies within the sublingual space medial to the mylohyoid muscle.
A diving ranula results from the rupture of a simple ranula which then extends posteriorly from the sublingual space into the submandibular space,
and can also extend anteriorly through a myelohyoid defect into the submandibular space.
The extension lacks an epithelial lining and is therefore classified as a pseudocyst.
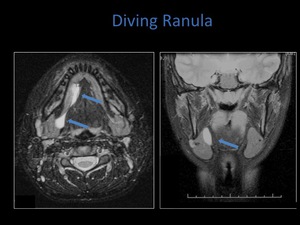
Fig. 13: Axial and coronal T2 fat sat sequences demonstrating a diving ranula.
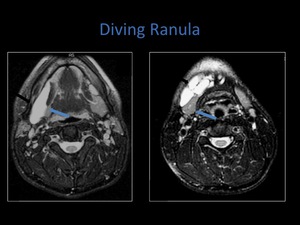
Fig. 14: Axial T2 fat sat sequences demonstrating a larger diving ranula. The second axial image show multiple septations within it.
Other cystic masses which occur in the floor of the mouth include dermoid and epidermoid cysts.
Retention cysts can also occur within the pharyngeal mucosal space.
They are typically smooth well circumscribed round or oval lesions.
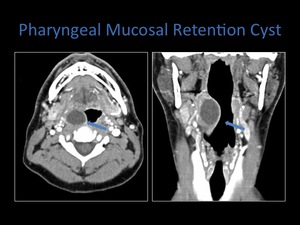
Fig. 15: Axial and coronal contrast enhanced CT demonstrating the nature of a pharyngeal mucosal retention cyst.
Benign Solid Neoplasms
The most common benign tumours of the major salivary glands are pleomorphic adenomas and Warthin tumours.
Pleomorphic adenomas occur most frequently within the parotid gland and are slightly more common in women in the fourth and fifth decades of life.
- Low signal on T1
- High signal on T2
- Enhance heterogenously
- Usually solitary and unilateral
- May undergo malignant transformation (rarely)
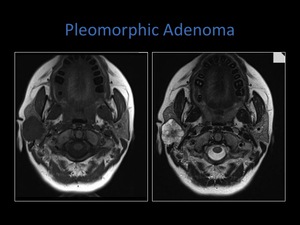
Fig. 16: Axial T1 and T2 MRI sequences demonstrating a pleomorphic adenoma within the right parotid gland; low signal on T1, high on T2.
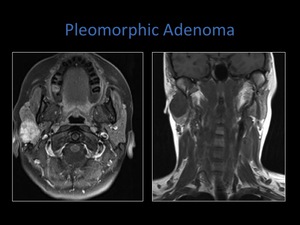
Fig. 17: Axial T1 fat sat MRI demonstrating heterogenous enhancement. Coronal T1 MRI.
Pleomorphic adenomas may also occur within the deep lobe of the parotid gand,
Iceburg tumour.
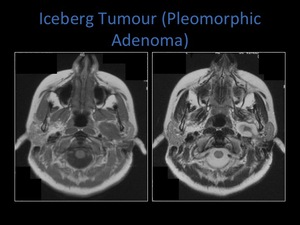
Fig. 18: Axial T1 and T2 MRI sequences demonstrating extension of a pleomorphic adenoma into the parapharyngeal space, known as an iceberg tumour.
Warthin tumour makes up 5-10% of benign salivary neoplasms.
They are more common in men in the fifth and sixth decades of life.
- T1 low signal
- T2 high signal,
contains solid and cystic elements
- Increased uptake of technetium pertechnetate
- 10%-60% bilateral
- Smoking is a risk factor
- Occur in the tail of the superficial lobe
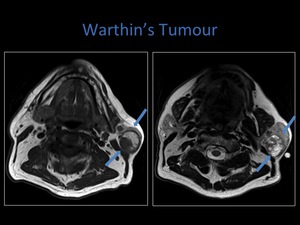
Fig. 19: Axial T1 and T2 MRI demonstrating a Warthin's Tumour within the left parotid gland.
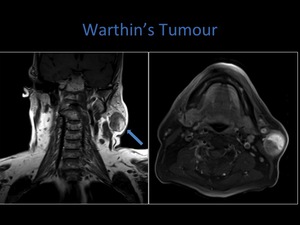
Fig. 20: Coronal T1 MRI demonstrating involvement of the parotid tail.
Intraparotid Lipoma
Lipomas are easily identified on imaging,
due to their characteristic features.
On CT they are well defined low attenuation lesions,
hyperechoic on ultrasound and T1 hyperintense on MRI.
The floor of the mouth is the third most common site for lipomas.
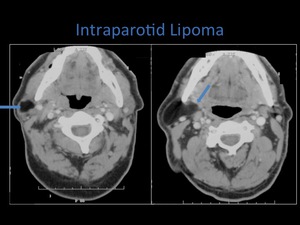
Fig. 21: Contrast enhanced Ct demonstrating a lipoma within the right parotid space.
Neoplastic Salivary Gland Disease
The smaller the salivary gland ,
the higher the rate of malignancy;
- 20-25% parotid gland
- 40-50 % submandibular gland
- 50-81% sublingual and minor salivary glands.
The most common malignancy of the parotid gland is mucoepidermoid carcinoma.
The most frequent malignancy of the submandibular gland is adenoid cystic carcinoma.
It is usually slow growing and has propensity for perineural spread.
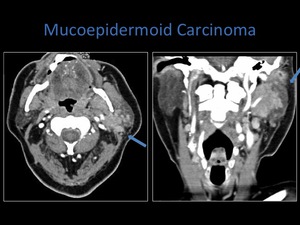
Fig. 22: Axial and coronal contrast enhanced CT. Note the the infiltrating nature of the lesion which extends to the carotid and parapharyngeal spaces. The coronal scan also demonstrates a metastatic lymph node.
Mucoepidermoid carcinoma occurs mostly in patients aged between 30-50 years.
It varies in levels of differentiation,
poorly differentiated being the most aggressive with increasing tendency to infiltrate.
Fig. 22
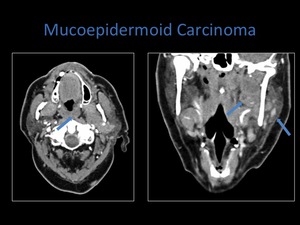
Fig. 23: Axial and coronal contrast enhanced CT demonstrating the lesion centered within the parotid space. However the coronal image demonstrates extension towards the foramen ovale within skull base.
Squamous cell carcinoma,
adenocarcinoma and acinic cell carcinoma of the salivary glands are less common.
Enlarged lymph nodes commonly accompany these tumours.
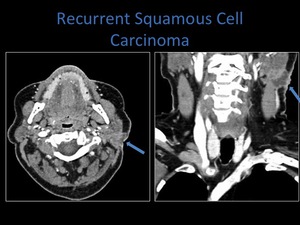
Fig. 24: Axial and coronal contrast enhanced CT. The patient had previous surgery for squamous cell carcinoma involving the parotid gland, these images demonstrate recurrence within the parotid space. Note the involvement of the skin.
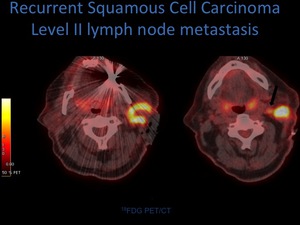
Fig. 25: Axial PET-CT images demonstrating FDG avid mass centered on the parotid gland, with an FDG avid metastatic lymph node evident on the right axial image.
The parotid gland contains lymphatic tissue,
the other salivary glands do not.
This occurs as it encapsulates late in the second trimester.
Lymphadenopathy may therefore also be seen within the parotid gland.
Similarily lymphoma may occur in the parotid gland,
either as primary lymphoma or an ifiltrative process.
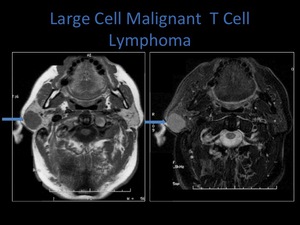
Fig. 26: Axial T1 and T2 fat sat sequences demonstrating a well defined mass within the superficial lobe of the right parotid gland, biopsy revealed T cell lymphoma.
Malignant tumours of the minor salivary glands may occur anywhere along the aerodigestive tract,
the minor salivary glands being associated with a higher rate of malignancy.
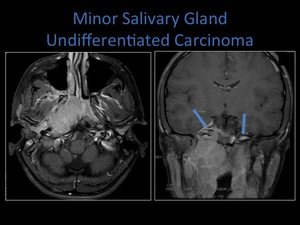
Fig. 27: Axial and coronal T1 post contrast MRI demonstrating an infiltrating tumour involving the nasopharynx, masticator and parapharyngeal spaces. Note the involvement of the right medial pterygoid muscle on the axial image. Coronal image shows tumour extension through the right foramen ovale and meningeal involvement. The foramen ovale is normal on the left.
