Learning objectives
In detection of prostate cancer,
transrectal ultrasound (TRUS) guided random biopsy is the “gold standard” in patients with high values of PSA (Prostatic Specific Antigen).
A new technique using MRI and US fusion imaging was considered by our institution to perform accurate targeted biopsies in highly suspicious areas of the peripheral prostate gland observed after MRI exam.
The aim of this study is to improve the accuracy of targeted biopsies and to increase the detection of prostatic cancer in patients with high PSA,
negative digital rectal exploration and negative previous random prostate biopsy.
Background
Prostate cancer is the most common cancer and the second most common cause of cancer deaths among men in the western countries [1].
The management of prostate cancer is a complex issue because of the difficulty in accurate staging and in predicting the speed of disease progression [2].
The current methods of prostate cancer detection include digital rectal examination (DRE),
serum prostate-specific antigen (PSA) level,
and transrectal ultrasound with random biopsy.
The role of MRI has evolved over the past decade with the development of newer techniques to localize,
stage,
and obtain functional information about the cancer.
Ninety-five percent of prostate cancers are adenocarcinomas that develop from the acini of the prostatic ducts.
They are classified according to Gleason score.
The prostate gland can be divided into 3 zones: peripheral,
central and transitional.
These zones are defined histologically and therefore many prostatic diseases have a zonal distribution.
70% of adenocarcinomas arise in the peripheral zone, 20% of adenocarcinomas arise in the transitional zone,
while only 10% of adenocarcinomas develop in the central zone [3].
Even in TRUS,
prostate can be divided into the same three zones,
but from echostructural point of view only two zones are well identified: peripheral and central zones.
The central zone comprises the posterior part of the gland and is often commonly heterogeneous in echotexture.
The peripheral zone forms most of the gland volume and it is described as isoechoic and homogeneous.
The transitional zone is the central part of the gland and it is hypoechoic.
The capsule is a hyperechoic structure that can be identified all around the prostate gland. [Fig.1].

Fig. 1: Transrectal ultrasound: axial scan of the prostate.
References: "Department of Radiology, San Bartolomeo Sarzana, Medical Hospital of Sarzana 2013."
Figure 1:Transrectal ultrasound: axial scan of the prostate.
In TRUS prostate cancer appears hypoechoic or isoechoic,
but most of time is hypoechoic.
Therefore,
TRUS is used primarily to direct the physician to suspicious areas in the prostate or to guide the performance of prostate biopsies.
Transrectal ultrasound–guided biopsy is the universally accepted method of confirming the presence of prostate cancer.
A randomized approach is used to obtain the biopsy samples because ultrasound has poor sensitivity for visualizing the tumor.
The yield from this approach varies[4,5].
In MRI the zonal anatomy of the prostate cannot be distinguished on T1-weighted images because the prostate appears to be of uniform intermediate signal intensity.
[Fig.
2]
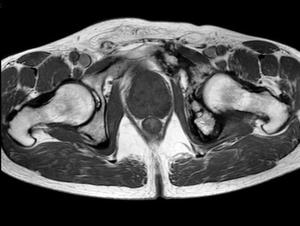
Fig. 2: TSE T1-weighted Ax image of the pelvis.
References: "Department of Radiology, San Bartolomeo Sarzana, Medical Hospital of Sarzana 2013."
Figure 2: TSE T1-weighted Ax image of the pelvis.
However,
the prostatic zones are well shown on T2-weighted images.[Fig 3]

Fig. 3: TSE T2-weighted Ax image of the pelvis
References: "Department of Radiology, San Bartolomeo Sarzana, Medical Hospital of Sarzana 2013."
Figure 3: TSE T2-weighted Ax image of the pelvis.
The anterior fibromuscular stroma is of low T1 and T2 signal intensity.
The peripheral zone has high T2 signal intensity similar to or greater than the signal of adjacent periprostatic fat.
The anatomic or true capsule surrounding the peripheral zone appears as a thin rim of low signal intensity on T2-weighted images [3,
6].
The central and transitional zones are both of lower T2 signal intensity than the peripheral zone,
possibly because of more compact smooth muscle and glandular elements.
There is also an age-related modification in the T2 signal intensity of the peripheral zone [7].
Prostate adenocarcinoma in the peripheral zone shows low signal intensity that is easily distinguished from the normal high-signal peripheral zone.
However,
low signal intensity in the peripheral zone is nonspecific and may be seen in benign conditions such as biopsy-related hemorrhage,
changes from hormone therapy,
prostatitis,
and postradiation fibrosis.
Therefore,
conventional MRI evaluation of prostate cancer,
that involves a combination of anatomic T1- and T2-weighted images,
is usually combined with one or more of several functional techniques such as diffusion-weighted imaging (DWI), dynamic contrast-enhanced MRI (DCE-MRI) and perfusion technique.
DWI is based on the principle of random molecular motion of water in tissues [8].
Healthy prostate tissue exhibits signal loss,
whereas areas of restricted molecular motion,
such as in densely packed tumor cells,
show higher signal and are therefore bright on the elevated b values DWI.
DWI reflects changes at the cellular level about tumor cellularity and cell membrane integrity.
The use of DWI enables the calculation of the apparent diffusion coefficient (ADC),
which is a value that measures water diffusion in tissues.
Movement of water is restricted in tumors,
leading to a reduction in the ADC value [9,
10].
After the acquisition of DWI images,
an ADC map,
which shows the ADC value of each voxel,
can be correlated with T2-weighted images.
DWI scans are characterized by the b value (in s/mm2),
which is a function of diffusion gradient strength.
DCE-MRI is based on the principle of tumor angiogenesis.
The values of contrast enhancement parameters such as mean transit time,
blood flow,
permeability of the surface area,
and interstitial volume are significantly greater in cancerous tissue than in normal tissue [11–12].
Relative peak enhancement is highly suspicious for prostate cancer in the peripheral zone and central zone [13].
