ECR 2013 / C-2388
Pyomyositis: MDCT and clinical correlation.
Congress:
ECR 2013
Poster Number:
C-2388
Type:
Scientific Exhibit
Keywords:
Musculoskeletal soft tissue, CT, Drainage, Infection
Authors:
G. C. Rivera Sierra1, J. A. Narváez2, J. Hernández Gañán3, M. M. Padilla Deza4, J. Quispe Bravo5, A. Pons Escoda6; 1L´Hospitalet de Llobregat (Barcelona) /ES, 2HOSPITALET DE LLOBREGAT/ES, 3L' Hospitalet de Llobregat/ES, 4Hospitalet de Llobregat, Ba/ES, 5L´Hospitalet de Llobregat (Barcelona) , ESP/ES, 6Barcelona/ES
DOI:
10.1594/ecr2013/C-2388
. Contrast-enhanced axial CT.")
Fig. 1:
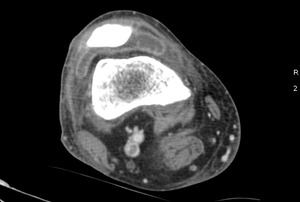
Case 2. Pyomyositis of bilateral paraspinal and both thighs at its invasive or...
. Contrast-enhanced axial CT.")
Fig. 2:
Case 2. Pyomyositis of bilateral paraspinal and both thighs at its invasive or...

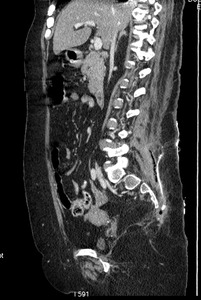
Fig. 3:
Case 2. Pyomyositis of bilateral paraspinal and both thighs at its invasive or...
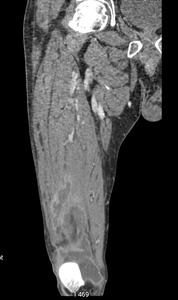
. Contrast-enhanced coronal CT.")
Fig. 4:
Case 2. Pyomyositis of bilateral paraspinal and both thighs at its invasive or...

Fig. 5:
Case 3. Pyomyositis of bilateral iliopsoas at its suppurative phase and...

Fig. 6:
Case 3. Pyomyositis of bilateral iliopsoas at its suppurative phase and...

Fig. 7:
Case 3. Pyomyositis of bilateral iliopsoas at its suppurative phase and...

Fig. 8:
Case 3. Pyomyositis of bilateral iliopsoas at its suppurative phase and...

Fig. 9:
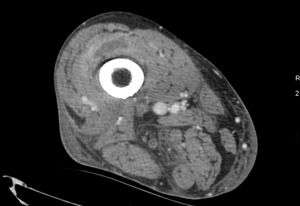
Case 5. Pyomyositis of right thigh at its suppurative phase, multifocal...

Fig. 10:
Case 5. Pyomyositis of right thigh at its suppurative phase, multifocal...

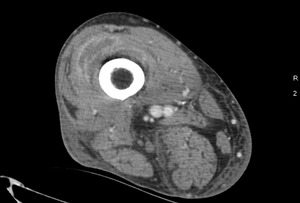
Fig. 11:
Case 5. Pyomyositis of right thigh at its suppurative phase, multifocal...

Fig. 12:
Case 5. Pyomyositis of right thigh at its suppurative phase, multifocal...

Fig. 13:
Case 7. Pyomyositis of bilateral paraspinal muscles at its suppurative phase,...

Fig. 14:
Case 7. Pyomyositis of bilateral paraspinal muscles at its suppurative phase,...

Fig. 15:
Case 9. Pyomyositis of right iliopsoas at its suppurative phase, with abscess...

Fig. 16:
Case 9. Pyomyositis of right iliopsoas at its suppurative phase, with abscess...

Fig. 17:
Case 10. Pyomyositis of right adductor at its suppurative phase, with abscess...

Fig. 18:
Case 10. Pyomyositis of right adductor at its suppurative phase, with abscess...

Fig. 19:
Case 11. Pyomyositis of left brachialis, coracobrachialis and biceps...

Fig. 20:
Case 11. Pyomyositis of left brachialis, coracobrachialis and biceps...

Fig. 21:
Case 11. Pyomyositis of left brachialis, coracobrachialis and biceps...

Fig. 22:
Case 11. Pyomyositis of left brachialis, coracobrachialis and biceps...

Fig. 23:
Case 11. Pyomyositis of left brachialis, coracobrachialis and biceps...

Fig. 24:
Case 11. Pyomyositis of left brachialis, coracobrachialis and biceps...

Fig. 25:
Case 15. Pyomyositis of left thigh at its suppurative phase, with abscess...

Fig. 26:
Case 15. Pyomyositis of left thigh at its suppurative phase, with abscess...

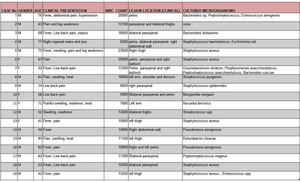
Table 1:
Underlying medical problems. M: male, F: female; DM: Diabetes mellitus, HCV:...

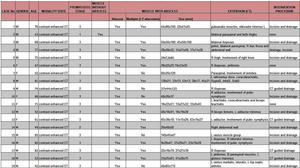
Table 2:
The demographic, clinical, laboratory and microbiology data.
M: male, F:...

Table 3:
Contrast-enhanced CT findings of affected muscle, extension and intramuscular...