1.
Imaging protocol
It is very important to start with a precise injury circumstances investigation followed by a careful clinical examination of the muscles.
An early post-injury d-HRUS between 2 and 48 h after the muscle trauma provides helpful information about any existing disturbance of the muscle structure,
particularly if there is any haematoma or if clinical examination points towards a functional disorder without evidence of structural damage.
MRI (after 48-72 hours post-injury) is mandatory for every injury which is suspicious for structural muscle injury.
MRI is helpful in determining whether oedema is present,
in what pattern,
and if there is a structural lesion including its approximate size.
Furthermore,
MRI is helpful in confirming the site of injury and any tendon involvement.
Then in our protocol an intermediate combined MRI - dHRUS follow-up has to be performed at about 2 weeks from the time of injury(monitoring the evolution of the healing process); in the end,
a last combined follow-up is performed at about 4-6 weeks from the injury time(assessing wheter or not there is a complete healing of the lesion and if scar tissue is present or not).
Commonly additional d-HRUS evaluation could be executed through the whole rehabilitation time in case of particular needs of the team medical staff.
Dynamic-HRUS
The US evaluation has to be conducted with high-quality linear transducers for the musculoskeletal study; it consists in multiple long-axis and short-axis scans of the region of interest of the injuried muscle(corrensponding to the region of pain),
assessing the potential structural damage,
the presence of intramuscular and/or intrafascial haematoma,
the status of the tendons,
the size of the tear and the possible scar tissue formation.
It is important not to make too much compression with the probe on the skin because a possible deep intramuscular hoematoma could be masked by the tissues mechanical compression and because a minor muscle injury could results less detectable.
Further a dynamic evaluation,
making the patient perform an isometric contraction of the muscle against appropriate resistance,
could be very useful in assessing minor injuries,
in appropriately giving the size of the lesion and,
particularly,
in evaluating the true stabilisation of the scar tissue during the follow-up of the lesion.
MRI
Fluid-sensitive sequences play an important role in our protocol for muscle injuries detection:
- Long axis plane: TSE T2W fat saturated,
STIR(long TE)
- sagittal if evaluating abnormalities in the anterior or posterior aspect of the thigh
- coronal if evaluating abnormalities in the medial or lateral aspect of the thigh
- Axial plane:TSE T1W and T2W or intermediate weighted (fat suppression increases sensitivity).
- Additional sequences:
- GE if looking for metallic foreign bodies,
gas,
hemosiderin- IV gadolinium in detecting early very subtle muscle injuries
- IV gadolinium in detecting early very subtle muscle injuries
2.
Soccer-related Imaging Findings
- DOMS (Delayed Onset Muscle Soreness)
MR: Diffuse hyprintensity of the whole muscle without signs of fibers tear US: No signs of fiber disruption or tissue disomogeneity
MR: Intramuscular 'feathery' hyperintensity on fluid-sensitive sequences without muscle fiber or tendon disruption
US: Areas of intramuscular hyperechogenicity and/or fibers focal disomogeneity Symptoms: Pain
MR: Hyperintensity (oedema and haemorrhage) intramuscularly or at the MTJ,
with extension along the fascial planes between muscle groups; Irregularity and mild laxity of tendon fibres; haematoma at the MTJ is pathognomonic
US: Discontinuity of muscle fibres with hypervascularity around disrupted muscle fibres; altered echogenicity and loss of perimysial striation adjacent to the MTJ; intramuscular fluid collection (hypoechogenicity) with a surrounding hyperechoic halo
Symptoms: Weakness
MR: Complete discontinuity of muscle fibres (at the MTJ) associated with extensive
oedema and haematoma,
and possible retraction of tendon
US: Ill-defined area of hyperechogenicity in the muscle,
which may cross fascial planes Symptoms: Loss of function
MR: T1-weighted and fluid-sensitive sequences may show hypo- to hyperintensity US: Area of intramuscular hyperechogenicity
Symptoms: Pain
MR: Redundant tendon edge lying within large fluid collection/haematoma; a small bony
fragment
US: Evaluation is difficult due to the presence of mixed echogenicity haematoma with similar echogenicity to the avulsed tendon
Symptoms: Loss of function
MR: Scar tissue formation appears hypointense on all pulse sequences with
progressively reduction of the nearby oedema signal intensity
US: Areas of scar tissue have irregular morphological features and display heterogeneous echo texture(mostly hyperechoic)
Symptoms: Normal function
- Acute (<48 h)
MR: typically isointense to muscles on T1-weighted images
US: Appears as a hypoechoic fluid collection and may contain debris
- Subacute
MR: higher signal intensity than muscle on both T1-weighted and fluid-sensitive sequences; variable signal intensities within hematoma
US: Variable appearance (anechoic,
hypoechoic or hyperechoic) within 24 h of injury; appearance changes over the next few days becoming hypoechoic or anechoic
- Chronic
MR: Dark signal intensity rim seen on all pulse sequences due to hemosiderin US: hypoechoic or anechoic.
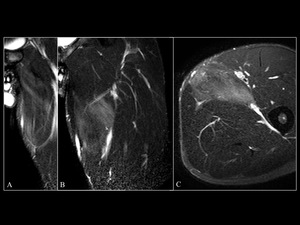
Fig. 8: DOMS. 25-year-old football player with delayed onset muscle soreness: diffuse hyperintensity is visible in the left adductor longus muscle. A and B: STIR long TE coronal scans; C: TSE T2W FATSAT axial scan. Notice the associated intraosseous hyperaemia against the pubic symphysis in A.

Fig. 9: I-II grade injury of the rectus femoris. 31-year-old football player with fibers disruption along the MTJ of the proximal tendon of the left rectus femoris muscle, surrounding intramuscular oedema and fascial hematoma. A: TSE T2 axial scan; B: STIR long TE coronal scan; C: STIR long TE sagittal scan.
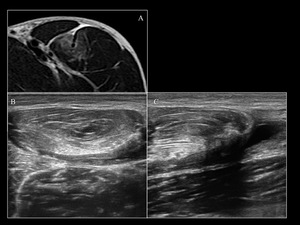
Fig. 10: Rectus Femoris Grade II. A: TSE T2W axial scan of the upper-middle third
of the thigh showing muscular tear at the rectus femoris MTJ and the intramuscular hematoma. B: Corresponding HRUS axial scan showing the hypoechoic tear, the intramuscular hematoma and the fascial involvment. C: Corresponding longitudinal scan highlining in particular the extension of the hematoma and the fibers architecture alteration.
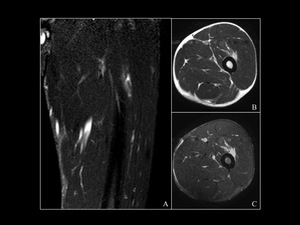
Fig. 11: II grade lesion of the vastus intermedius. 28-year-old football player with fibers disruption and intramuscular hematoma in the deep portion of the left vastus intermedius. A: STIR long TE coronal scan; B: TSE T2W axial scan; C: TSE T2W FATSAT axial scan
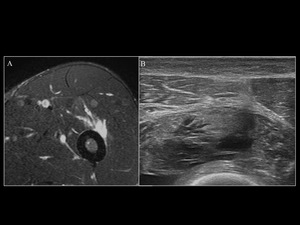
Fig. 12: Vastus intermedius Grade II. A: TSE T2W FATSAT axial scan of the upper- middle thigh; II grade vastus intermedius muscle tear with intramuscular hematoma seen as hyperintensity around the lesion. B: Corresponding HRUS axial scan through the deep portion of the vastus intermedius showing the hypoechoic fibers interruption with hematoma and adiacent fibers disomogeneity.
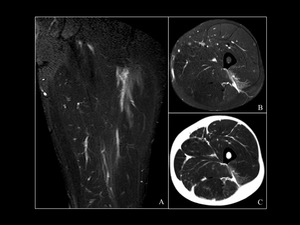
Fig. 13: I-II grade lesions of the vastus lateralis muscle. 25-year-old football player
with myofascial oedema at the upper-middle third of the left vastus lateralis muscle. MR performed 24h post-trauma. A: STIR long TE coronal scan; B: TSE T2W FATSAT axial scan C: TSE T2W axial scan
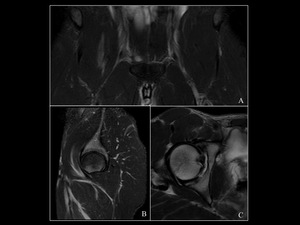
Fig. 14: II grade lesion of the Iliopsoas muscle. Fibers disruotion with intramuscular oedema visible at the MTJ of the right ilio-psoas muscle. A: STIR long TE coronal scan; B: STIR long TE sagittal scan. C: TSE T2W FATSAT axial scan
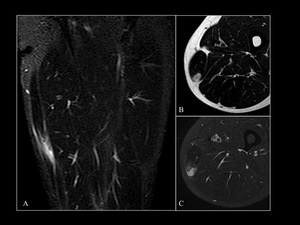
Fig. 15: Grade II lesion of the Gracilis muscle. 31-year-old football player with fibers disruption on the middle-distal third of the left gracilis muscle with intramuscular oedema and fascial involvment. A: STIR long TE coronal scan B: TSE T2W axial scan C: TSE T2W FATSAT axial scan
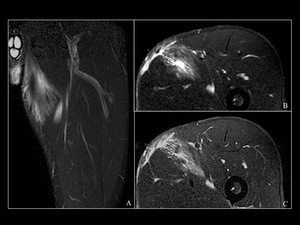
Fig. 16: II grade adductor longus tear. 29-year-old football player with re-injury of the left adductor longus muscle. Images show the hyperintense hematoma extending from the previous myofascial tear superficial site, through the myofascial plane( between adductor longus and brevis), into the deep portion of the thigh. A: STIR long TE sagittal scan; B: TSE T2W FATSAT upper axial scan; C: TSE T2W FATSAT lower axial scan.
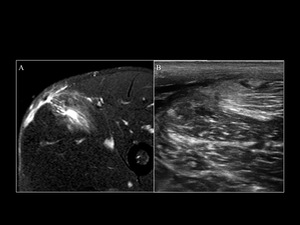
Fig. 17: Adductor longus Grade II. A: TSE T2W FATSAT axial scan of the upper portion of the thigh. Grade II tear on a previous myofascial lesion of the adductor longus muscle. The tear appears as a loss of signal image and the intra- and inter- muscular hematoma as a hyperintense signal on this scan. B: Corresponding HRUS scan showing the hypoechoic fibers tear, the more superficial scar tissue formation at the previous lesion site, the hyperechoic intramuscular hematoma and the hypoechoic fascial hematoma.
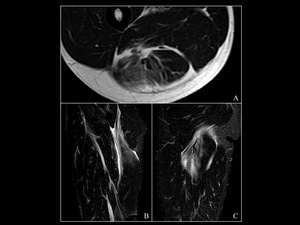
Fig. 18: II grade lesion of the hamstrings. 24-year-old footbal player with laceration of the fibers at the MTJ of the right biceps femoris/semitendineous muscle with intra- and inter-muscular hematoma extending along the fascia and surrounding the sciatic nerve. A: TSE T2W axial scan; B: STIR long TE sagittal scan; C: STIR long TE coronal scan.
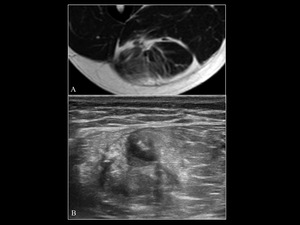
Fig. 19: Hamstrings Grade II tear. A: TSE T2W axial scan of the upper-middle thigh. Fibers tear at the proximal MTJ of the right biceps femoris/semitendineous muscle with intra- and inter-muscular hematoma extended along the fascia and surrounding the sciatic nerve. B: Corresponding HRUS axial scan showing the hypoechoic fibers tear with intramuscular hematoma extending towards the fascia and the surrounding muscular fibers disomogeneity.
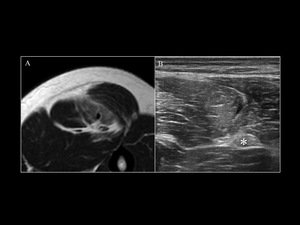
Fig. 20: Hamstrings Grade II. A: TSE T2W axial scan passing through the middle third of the thigh; the image shows a partial tear of the fibers at the MTJ of the right semitendinosus muscle with associated intramuscular oedema. B: Corresponding HRUS axial scan showing the tear on the lateral side of the semitendinosus muscle with surrounding hyperechoic oedema; * : sciatic nerve.
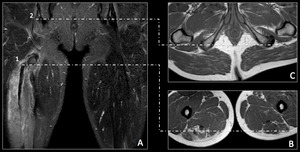
Fig. 21: Hamstrings conjoined tendon avulsion. A) Coronal STIR long TE SENSE sequence showing diffuse muscle edema and conjoined tendon avulsion from the ischial tuberosity (1) and the tendon stump at the middle third of the thigh (2). B) Axial T1W TSE HR SENSE sequence at ischial tuberosity level. C) Axial T1W TSE HR SENSE at middle third of the thigh.
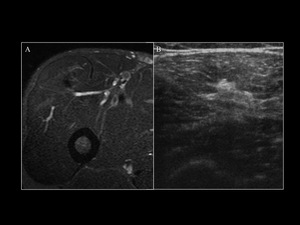
Fig. 22: Rectus femurs scar. A: TSE T2W FS axial scan of the upper- middle portion of the thigh shows the formation of hypointense scar tissue of an old
II grade tear into the deep part of the right rectus femoris muscle; B: Corresponding HRUS axial scan of the same region showing the scar tissue into the deep part of the rectus femoris muscle as a hyperechoic focal tissue disomogeneity.









, into the deep portion of the thigh. A: STIR long TE sagittal scan; B: TSE T2W FATSAT upper axial scan; C: TSE T2W FATSAT lower axial scan.")




 Coronal STIR long TE SENSE sequence showing diffuse muscle edema and conjoined tendon avulsion from the ischial tuberosity (1) and the tendon stump at the middle third of the thigh (2). B) Axial T1W TSE HR SENSE sequence at ischial tuberosity level. C) Axial T1W TSE HR SENSE at middle third of the thigh.")
