ECR 2014 / C-0897
CT Angiography collateral flow score in acute stroke patients with M1 or M2 thrombosis: A reproducible and practical predictor of infarct size
This poster is published under an open license. Please read the disclaimer for further details.
Congress:
ECR 2014
Poster Number:
C-0897
Type:
Scientific Exhibit
Keywords:
Neuroradiology brain, CT-Angiography, MR, Thrombolysis, Acute
Authors:
J. A. Gadde, K. Anzilotti, X. Liu, A. Liu; Newark, DE/US
DOI:
10.1594/ecr2014/C-0897

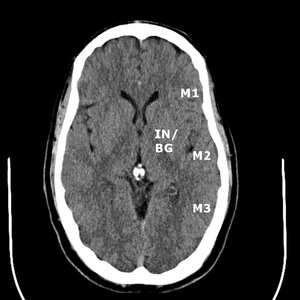
Fig. 1:
ASPECTS territories for the middle cerebral artery distribution.

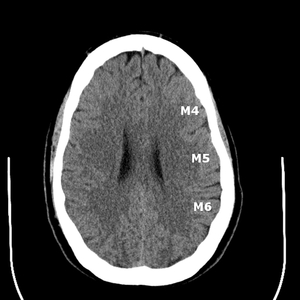
Fig. 2:
ASPECTS territories for the middle cerebral artery distribution.

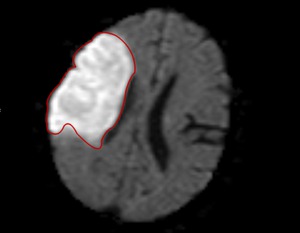
Fig. 3:
Measurement of infarct volume using the diffusion weighted sequence of an MRI.