ECR 2014 / C-1004
CT-analysis of acetabular component position in mechanically guided vs free-hand anatomical-landmarks techniques.
This poster is published under an open license. Please read the disclaimer for further details.
Congress:
ECR 2014
Poster Number:
C-1004
Type:
Educational Exhibit
Keywords:
Prostheses, Surgery, Outcomes analysis, CT, Pelvis, Musculoskeletal joint, Bones
Authors:
E. S. Lomtatidze1, M. D. Abakirov1, A. A. Dedyurin1, O. M. Urvantseva1, A. Albluwi2, A. R. Sarukhanyan1, Y. Borisov1; 1Moskow/RU, 2Moscow /RU
DOI:
10.1594/ecr2014/C-1004
:631. DOI: 10.3928/01477447-20100722-22")
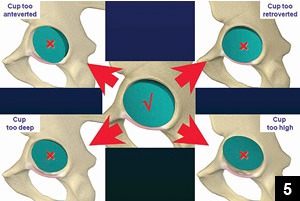
Fig. 1:
The concept of Beverland et al. [13] The central diagram is the ideal...

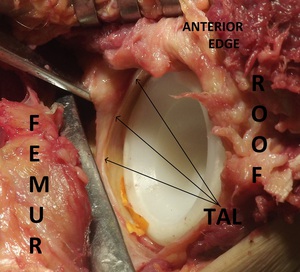
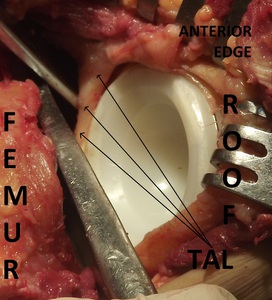
Fig. 2:
Acetabular component is in optimal position. Intraoperative view. Patient is in...

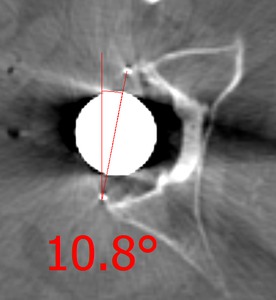
Fig. 3:
Axial CT-scan. AAA=10.8° Cup is inside the “safe zone”.

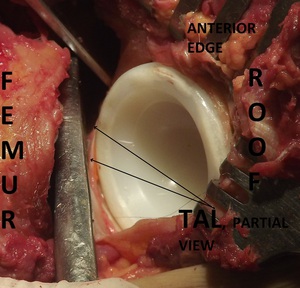
Fig. 4:
Intraoperative view. Patient is in the lateral decubitus position. The hip is...

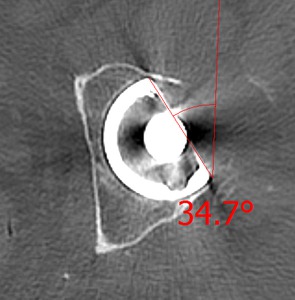
Fig. 5:
Axial CT-scan. AAA=34.7° Cup is in excessive anteversion.
. Acetabular component is too retroverted.")
Fig. 6:
Intraoperative view. Patient is in the lateral decubitus position. The hip is...

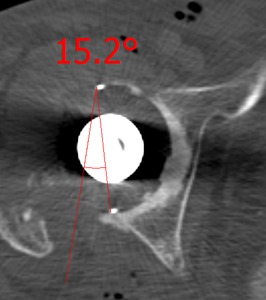
Fig. 7:
Axial CT-scan. Acetabular version angle=-15.2° Cup is in retroversion.