Normal pregnancy
MRI appearance of normal pregnancy at 5 weeks’ gestation is shown in figure 1,
and the corresponding TVUS image and anatomic scheme are presented in figure 2.
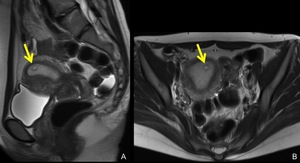
Fig. 1: MRI of normal pregnancy at 5 weeks’ gestation.
In thickened endometrium, a cystic structure (arrows) with thick wall is identified, this is a normal gestational sac on MRI.
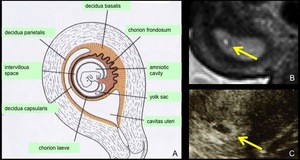
Fig. 2: A. Scheme of the GS-like structure. B, C. MRI and US appearance of the GS-like structure. The wall of the GS-like structure on T2-weighted MRI (B, arrow) and “high echogenic rim” on TVUS (C, arrow) correspond to the chorionic villi and decidua. The cystic space corresponds to the amniotic cavity and intervillous space.
References: A: Sadler et al. (2004) Lippincott Williams & Wilkins, Langman's medical embryology 9th edition (revised) B,C. Radiology, Kobe City Medical Center General Hospital - Kobe/JP
Tubal pregnancy
Tubal pregnancy is a pregnancy that occurs within the fallopian tube,
and it is the most common form of ectopic pregnancy,
accounting about 98% of all ectopic pregnancies.
The most common implantation site is the ampulla (75-80%),
followed by the isthmus (10-15%) and the fimbria (5%),
the interstitial (2-4%) (figure 3) [4,6].
There are several therapeutic options such as laparoscopic salpingectomy or salpingotomy,
and medical treatment,
etc.
depending on patients’ clinical conditions [7].
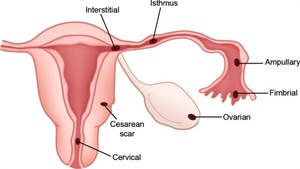
Fig. 3: Implantation site of ectopic pregnancy.
References: Edward PL et al. (2008) Diagnostic Clues to Ectopic Pregnancy. RadioGraphics 28:1661–1671
Imaging finding of tubal pregnancy
On TVUS,
findings suggesting tubal pregnancy are an adnexal mass with or without yolk sac or living embryo,
hyperechoic ring surrounding an extrauterine gestational sac (tubal ring sign,
figure 4-A),
peripheral hypervascurality around the hyperechoic ring (ring of fire sign,
figure 4-B).
Identifying living embryo is the most specific finding of tubal pregnancy,
however,
it does not have high sensitivity [8].
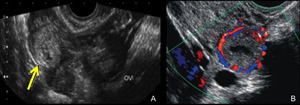
Fig. 4: TVUS findings of tubal pregnancy. A. TVUS of the right adnexa reveals an extraovarian adnexal mass with a hyperechoic tubal ring (arrow). OV = right ovary. B. Transvaginal color Doppler US images of a tubal pregnancy show peripheral hypervascularity surrounding the extrauterine gestational sac.
References: Edward PL et al. (2008) Diagnostic Clues to Ectopic Pregnancy. RadioGraphics 28:1661–1671
CT is not the first choice for imaging in patients suspected ectopic pregnancy,
but sometimes performed suspecting other diseases.
Contrast-enhanced CT can demonstrate hemoperitoneum with or without extravasation of contrast medium around uterus (figure 5).
CT has low soft tissue resolution compared to MRI,
so demonstrating GS-like structures is usually difficult.
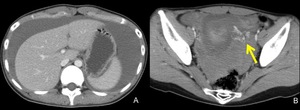
Fig. 5: CT of a patient with ectopic pregnancy.
A,B. contrast-enhanced CT shows massive hemoperitoneum, and extravasation of contrast medium (B, arrow).
This patient had artificial abortion several weeks before and villous tissue was identified. After arriving our hospital, left salpingectomy was performed and tubal pregnancy was confirmed, and diagnosed as heterotopic (intra and extrauterine) pregnancy.
MRI has excellent soft tissue resolution,
and very useful for evaluating gynecological disorders,
also for ectopic pregnancy.
Previously reported MRI findings of tubal pregnancy are as follows [2,3,4,5,9].
・The GS-like structure in the fallopian tube (figure6-9).
A cystic lesion with intensely enhanced thick wall can be found.
The wall shows high intensity on T2-weighted images containing distinct
low intensity.
・Tubal wall enhancement (figure 10).
This finding is thought to reflect increased vascurality of the tubal wall.
・Tubal wall dilatation with hemosalpinx (figure 10).
・Intensely enhanced papillary projection in the fallopian tube (figure 10).
This finding corresponds to the placental tissue in the tube.
Hemoperitoneum is also seen,
but this is a relatively nonspecific finding compared with other findings.
By studying following two cases of tubal pregnancy,
the imaging of what we call the GS-like structure and its pathological findings can be learned.
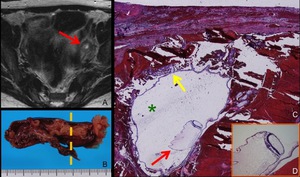
Fig. 6: A case of left tubal pregnancy at 7 weeks’ gestation.
A. Axial T2-weighted MRI shows a GS-like structure (arrow), which is a cystic lesion with thick wall.
B. Photograph of left fallopian tube. Dilated tube with hemosalpinx was found.
C, Photomicrograph (hematoxylin-eosin stain) of the cut surface along the broken line in Fig. B. Fetus (red arrow) inside chorionic membrane (yellow arrow) is found. Cystic portion of the GS-like structure is also demonstrated (green asterisk). Hemorrhage in the wall of the tube is found.
D. Magnification of the fetus shows nerve tissue.
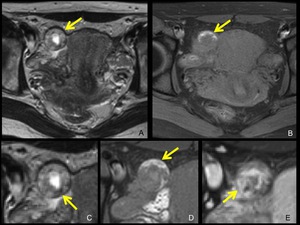
Fig. 7: Right tubal pregnancy of 6 weeks’ gestation.
A,B. Axial T2-weighted (A), and fat-suppressed T1-weighted (B) MRI show a GS-like structure (arrow) lateral to the uterus.
C,D,E. Magnification of the GS-like structure of axial T2-weighted (C), fat-suppressed T1-weighted (D), gadolinium-enhanced fat-suppressed T1-weighted (E) MRI are shown.
In the relatively thick wall of the GS-like structure, low intensity area on T2-weighted MRI (C, arrow) and high intensity area on T1-weighted MRI (D, arrow) is identified, which suggest hemorrhage in the wall.
The wall is strongly enhanced (E, arrow).

Fig. 8: A. Photograph of the right fallopian tube. Hematoma and villous tissue in the enlarged isthmus of the fallopian tube is shown (arrow).
B,C. Photomicrograph (hematoxylin-eosin stain) of the cut surface along the broken line in Fig. A is shown in Fig. B,C. Hemorrhage in the wall (B, yellow arrow) of the tube is observed. Villi (C, arrow) invading the tubal wall is demonstrated.
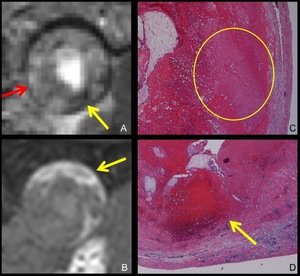
Fig. 9: MRI and pathological findings of the GS-like structure.
A,B. Magnification of the GS like structure on T2-weighted (A), and fat-suppressed T1-weighted (B) MRI. A GS-like structure is typically a cystic lesion with relatively thick wall.
On T2-weighted MRI, its wall shows high intensity (A, red arrow) and contains distinct low intensity area (A, yellow arrow). On fat-suppressed T1-weighted MRI, part of the wall shows high intensity (B, arrow).
C,D. Photomicrograph (hematoxylin-eosin stain) of the wall of the GS-like structure demonstrates edematous change (C, circle) and hemorrhagic change (D, arrow) of the wall.
These findings can explain the MRI findings.
This is one of the useful findings to differentiate a GS-like structure from a corpus luteum cyst.
Figure 10 is MRI of a patient of right tubal pregnancy.
In this case,
tubal wall enhancement,
tubal wall dilatation with hemosalpinx,
and intensely enhanced papillary projection in the fallopian tube can be found.
Intraoperative photograph of this patient is shown in figure 11.
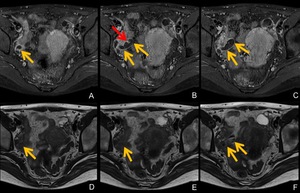
Fig. 10: MRI of right tubal pregnancy at 7 weeks’ gestation.
A,B,C. Axial gadolinium-enhanced fat-suppressed T1-weighted MRI show dilated fallopian tube (A,B,C, yellow arrows) with its wall enhanced intensely. Note intensely enhanced papillary projection in the fallopian tube (B, red arrow).
D,E,F Axial T2-weighted MRI demonstrate contents of dilated fallopian tube (D,E,F, yellow arrows), which show heterogeneously low signal suggesting hematoma.
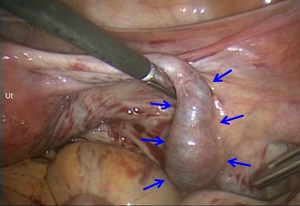
Fig. 11: Intraoperative photograph of right tubal pregnancy.
Dilated right fallopian tube due to hemosalpinx is found (arrows). Ut: Uterus
Corpus luteum cyst
A corpus luteum cyst occurs after an egg has been released from a follicle,
and usually breaks down and disappears in about 14 days,
however,
when a pregnancy occurs,
it produces progesterone by about 9 weeks’ gestation when a placenta begins to produce progesterone.
From about 12 weeks’ gestation,
a corpus luteum cyst begins to involute [10,11].
So,
in the early gestation,
distinction from a GS-like structure may be problematic.
A corpus luteum cyst is a cystic lesion with thick wall.
Its wall shows slightly increased intensity on T1-weighted images and relatively low intensity on T2-weighted images [12],
and it is enhanced intensely.
These findings are similar to a GS-like structure,
and sometimes it is difficult to differentiate them (figure 12,13). Unlike a GS-like structure,
distinct low intensity area suggesting hemorrhage can not be found in the wall of a corpus luteum cyst.
And it is located in the ovary,
so follicular cysts often can be found around it.
Thinking of the low incidence of ovarian pregnancy,
the localization of the corpus luteum cyst is thought to be the most useful finding.
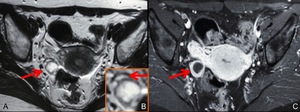
Fig. 12: MRI of a corpus luteum cyst.
A,B. Axial T2-weighted MRI (A) and magnification of a corpus luteum cyst (B) show cystic lesion (A, arrow) with thickened wall in the right ovary. Around the cystic lesion, several small cysts (B, arrow) representing follicular cysts are found, and this finding suggests that the lesion is a corpus luteum cyst.
C. Axial gadolinium-enhanced fat-suppressed T1-weighted MRI shows the corpus luteum cyst (arrow) with its wall strongly enhanced, and this finding is identical with a GS-like structure.
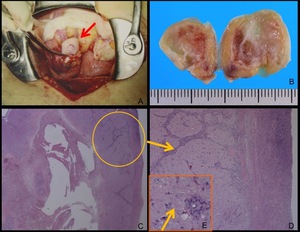
Fig. 13: A. Intraoperative photograph. A whitish cystic lesion (A, arrow) was found at the periphery of the right ovary.
B. Macroscopic photograph shows the cystic lesion with whitish or slightly yellowish wall, which is compatible with a corpus luteum cyst.
C,D. Photomicrograph (hematoxylin-eosin stain) of the corpus luteum cyst.
Figure D is the magnification of the wall. Most of the wall consists of granulosa lutein cells with clear cytoplasm.
At the periphery of the wall, Theca cells form dendritic projection. Granulosa lutein cells (E, arrow) contain fat in their cytoplasm, so corpus luteum cysts usually have macroscopically yellowish appearance.
Hemorrhage in a corpus luteum cyst after abortion sometimes can be similar to ectopic pregnancy clinically (figure 14,15).
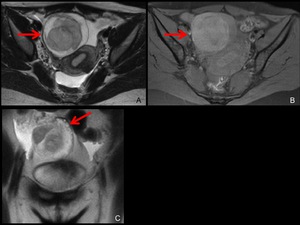
Fig. 14: MRI of the hemorrhage in a corpus luteum cyst after spontaneous abortion.
This patient with positive hCG and hematoma at the right adnexa on TVUS was suspected of the rupture of right tubal pregnancy.
A,B. Axial T2-weighted (A) and fat-suppressed T1-weighted (B) MRI show hematoma (A,B, arrow) at the right adnexa.
C. Coronal T2-weighted MRI (C) reveals small cysts (C, arrow) around the hematoma. This finding suggests the hematoma is located in the ovary.
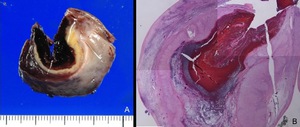
Fig. 15: Pathological findings of the hemorrhagic corpus luteum cyst.
A. Photograph of the resected corpus luteum cyst shows hematoma in the thick yellowish wall.
B. Photomicrograph (hematoxylin-eosin stain) shows granulosa lutein cells in the wall, and no evidence of ectopic pregnancy.
Interstitial pregnancy
Interstitial pregnancy is defined as the implantation at the proximal part of the fallopian tube,
which is embodied within the muscular wall of the uterus [6]. Interstitial pregnancy is relatively rare condition,
and occurs in 2-4% of all tubal pregnancies [13].
With development of assisted reproductive technology and increasing number of patients of sexually transmitted diseases,
the prevalence of interstitial pregnancy is rising [14].
Interstitial pregnancy is associated with high risk of massive uncontrollable hemorrhage,
and early diagnosis is mandatory.
However,
early diagnosis of this condition is sometimes challenging,
since it can be occasionally misdiagnosed as normal intrauterine pregnancy or angular pregnancy,
and the patients tend to have mild symptoms such as lower abdominal pain initially [6].
As with other ectopic pregnancies,
the diagnosis is performed by elevated hCG level and TVUS.
MRI is useful in showing precise anatomic structures for the correct diagnosis,
and distinguishing from intrauterine pregnancy (figure 16-18) [6].
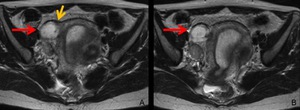
Fig. 16: MRI of interstitial pregnancy at 6 weeks’ gestation.
The endometrium is thickened and no sign of intrauterine pregnancy is found. A GS-like structure is identified lateral to the right cornus (A,B, red arrow), and the junctional zone is uninterrupted.
The myometrium embodies the GS-like structure (A, yellow arrow), this finding facilitates differentiating from ectopic pregnancy within the tubal isthmus.
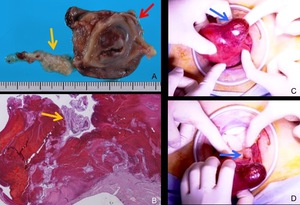
Fig. 17: Pathological and intraoperative findings of interstitial pregnancy.
Partial resection of the right uterine cornus, and isthmus of fallopian tube was performed.
A. Photograph of the uterine cornus (red arrow) and isthmus of fallopian tube (yellow arrow).
B. Photomicrograph (hematoxylin-eosin stain) shows villous tissue (arrow) invading myometrium. Around the implantation site, massive hemorrhage is found.
C,D. Intraoperative photographs of left interstitial pregnancy (another case) show a dark red mass at the interstitial portion of the fallopian tube (C, arrow). Left ovary is identified (D, arrow).
The patient in figure 18 is a case of normal pregnancy,
however,
suspected of interstitial pregnancy on TVUS. As with this case,
some normal pregnancy cases are difficult to differentiate from interstitial pregnancy by TVUS.
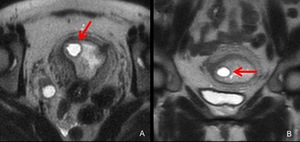
Fig. 18: MRI was performed suspecting interstitial pregnancy by TVUS at 5 weeks’ gestation.
A,B. Axial (A) and coronal (B) T2-weighted MRI show a GS-like structure (arrows) at the right cornus and it is located inside the junctional zone.
Cervical pregnancy
Cervical pregnancy is defined as the implantation in the uterine endocervix.
This condition is extremely rare,
and occurs no more than 1% [15].
Risk factors of this condition is past history of intrauterine curettage,
cesarean delivery,
pelvic inflammatory disease,
assisted reproductive technology [16],
etc. As with other ectopic pregnancy,
early diagnosis and treatment is essential.
Treatment option is systemically or locally administered Methotrexate,
dilatation and curettage,
uterine artery embolization and surgical therapy [17].
Distinction from ongoing abortion is sometimes difficult,
and presence of vascurality of the GS-like structure observed in TVUS or MRI may be helpful (figure 19,20).
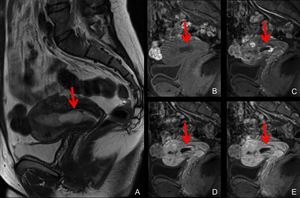
Fig. 19: MRI of cervical pregnancy at 6 weeks’ gestation.
A. Sagittal T2-weighted MRI shows thickened endometrium and a GS-like structure at the uterine cervix.
B,C,D,E. Sagittal, dynamic gadolinium-enhanced fat-suppressed T1-weighted MRI (B: precontrast, C: 30 seconds D: 60seconds E:120 seconds) demonstrate marked vascurality of the GS-like structure (arrows).
Uterine artery embolization was performed followed by dilatation and curettage.
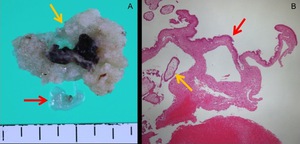
Fig. 20: Pathological findings of cervical pregnancy.
A. Photograph shows the fetus (red arrow) and villous tissue (yellow arrow).
B. Photomicrograph (hematoxylin-eosin stain) shows villous tissue (yellow arrow) and the epithelium of the cervix (red arrow).
Ovarian pregnancy
Ovarian pregnancy is defined as the implantation in the ovary.
The incidence is reported approximately 0.5-3.0% of all ectopic pregnancies [4].
This condition is associated with neither pelvic inflammatory disease nor infertility,
and its association with intrauterine device is known.
Patients of teenager are relatively few unlike tubal pregnancy.
Distinction between ovarian pregnancy and a corpus luteum cyst may be difficult due to its location.
Characteristic finding of GS-like structures above mentioned may be helpful for their distinction.
Figure 21,22 are TVUS and pathological findings of ovarian pregnancy.
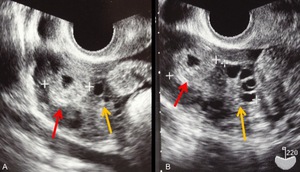
Fig. 21: TVUS images of ovarian pregnancy at 5 weeks’ gestation.
A,B. TVUS images show a GS-like structure (red arrow), just in touch with right ovary (yellow arrow).
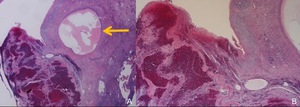
Fig. 22: Pathological findings of ovarian pregnancy.
A,B. Photomicrograph (hematoxylin-eosin stain) of ovarian pregnancy.
Inside the ovarian stroma, hemorrhagic villi and trophoblast cells are identified. No evidence of tubal pregnancy is found. Follicle of the ovary (A, arrow) is shown.
Cesarean scar pregnancy
Cesarean scar pregnancy is defined as the implantation at the site of the incision of previous cesarean delivery.
The incidence of cesarean scar pregnancy is approximately 0.15% of pregnancies of previous cesarean delivery [18].
More patients are reported in association with increasing number of cesarean delivery.
This condition may lead to severe complications,
such as uterine rupture and severe hemorrhage,
and early diagnosis and treatment is mandatory. There are several treatment options,
depending on patients’ clinical conditions.
Systemically or locally administered methotrexate,
dilatation and curettage,
excision of trophoblastic tissues using either laparotomy or laparoscopy,
and more recently uterine artery embolization are reported [17].
MRI is useful demonstrating the implantation site.
The GS-like structure is located in the lower anterior wall of uterus corresponding cesarean scar.
The myometrium at the implantation is markedly thin (figure 23) [4].
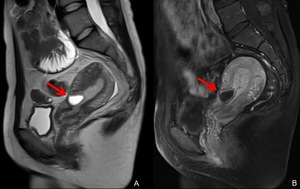
Fig. 23: MRI of cesarean scar pregnancy.
A. Sagittal T2-weighted MRI shows a GS-like structure (arrow) at the cesarean scar. The uterine myometrium of the implantation site is markedly thin.
B. Sagittal gadolinium-enhanced fat-suppressed T1-weighted MRI shows the enhanced GS-like structure (arrow).
Abdominal pregnancy
Abdominal pregnancy is defined as the implantation within the peritoneal cavity outside the fallopian tube or ovary and not located in the broad ligament.
This condition is extremely rare and occurs approximately 1% of all ectopic pregnancies [15]. The most common implantation site is Douglas‘ pouch,
followed by vesicouterine pouch,
uterosacral ligament,
round ligament.
Reported extrapelvic implantation site is omentum,
liver,
spleen,
diaphragm [4],
etc.
Abdominal pregnancy is classified into primary and secondary abdominal pregnancy.
Primary abdominal pregnancy is a pregnancy that implanted directly in the abdominal cavity and its organs,
and this is extremely rare.
Typically an abdominal pregnancy is a secondary pregnancy which means that it originated from a tubal or ovarian pregnancy and re-implanted [19].
Risk factors are assisted reproductive technology,
damage of fallopian tube,
pelvic inflammatory disease,
and endometriosis,
etc. Treatment is usually surgical therapy,
however,
depending on the implantation site and clinical conditions,
Methotrexate administration is selected [20].
Imaging finding is identification of a GS-like structure at the implantation site.
When the implantation site is uncertain in a case of suspected abdominal pregnancy,
contrast-enhanced CT may be useful because of its capability of wide range images in short time.
Two cases of abdominal pregnancy are presented (figure 24-27).
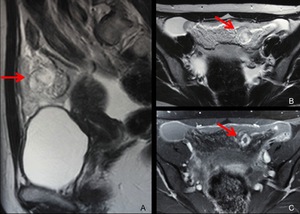
Fig. 24: MRI of abdominal pregnancy (omentum) at 6 weeks’ gestation.
A. Sagittal T2-weighted MRI shows a GS-like structure (arrow) in the omentum.
B,C. Axial T2-weighted (B) and gadolinium-enhanced fat-suppressed T1-weighted MRI show the GS-like structure (B,C, arrow) and hemoperitoneum.
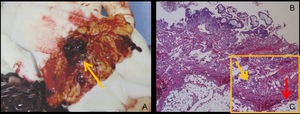
Fig. 25: A. Intraoperative photograph.
The GS-like structure covered with hematoma (arrow) was identified in the omentum, and resected.
B,C. Photomicrograph (hematoxylin-eosin stain) of the pregnancy.
Trophoblast cells (yellow arrow) invading omentum (red arrow) are found, which indicates this is the implantation site. Extensive hematoma around the lesion is also found.
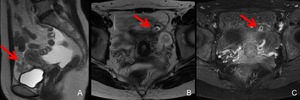
Fig. 26: MRI of abdominal pregnancy (vesicouterine pouch) of 6 weeks’ gestation.
A. Sagittal T2-weighted MRI shows hematoma (arrow) in the vesicouterine pouch.
B,C. Axial T2-weighted (B) and gadolinium-enhanced fat-suppressed T1-weighted (C) MRI show a GS-like structure (arrows) inside the hematoma in the vesicouterine pouch.
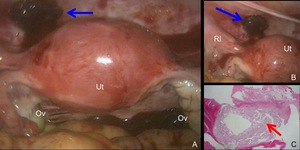
Fig. 27: Intraoperative photograph and pathological finding of abdominal pregnancy (vesicouterine pouch).
A. Intraoperative photograph shows a mass covered with hematoma (arrow) at the vesicouterine pouch. Ut: uterus, Ov: ovary
B. Magnification of the implantation site. Rl: round ligament
C. Photomicrograph (hematoxylin-eosin stain) demonstrates villous tissue (arrow).

 with thick wall is identified, this is a normal gestational sac on MRI.")
 and “high echogenic rim” on TVUS (C, arrow) correspond to the chorionic villi and decidua. The cystic space corresponds to the amniotic cavity and intervillous space. References: A: Sadler et al. (2004) Lippincott Williams & Wilkins, Langman's medical embryology 9th edition (revised) B,C. Radiology, Kobe City Medical Center General Hospital - Kobe/JP")
 Diagnostic Clues to Ectopic Pregnancy. RadioGraphics 28:1661–1671")
. OV = right ovary. B. Transvaginal color Doppler US images of a tubal pregnancy show peripheral hypervascularity surrounding the extrauterine gestational sac. References: Edward PL et al. (2008) Diagnostic Clues to Ectopic Pregnancy. RadioGraphics 28:1661–1671")
.
This patient had artificial abortion several weeks before and villous tissue was identified. After arriving our hospital, left salpingectomy was performed and tubal pregnancy was confirmed, and diagnosed as heterotopic (intra and extrauterine) pregnancy.")
, which is a cystic lesion with thick wall.
B. Photograph of left fallopian tube. Dilated tube with hemosalpinx was found.
C, Photomicrograph (hematoxylin-eosin stain) of the cut surface along the broken line in Fig. B. Fetus (red arrow) inside chorionic membrane (yellow arrow) is found. Cystic portion of the GS-like structure is also demonstrated (green asterisk). Hemorrhage in the wall of the tube is found.
D. Magnification of the fetus shows nerve tissue.")
, and fat-suppressed T1-weighted (B) MRI show a GS-like structure (arrow) lateral to the uterus.
C,D,E. Magnification of the GS-like structure of axial T2-weighted (C), fat-suppressed T1-weighted (D), gadolinium-enhanced fat-suppressed T1-weighted (E) MRI are shown.
In the relatively thick wall of the GS-like structure, low intensity area on T2-weighted MRI (C, arrow) and high intensity area on T1-weighted MRI (D, arrow) is identified, which suggest hemorrhage in the wall.
The wall is strongly enhanced (E, arrow).")
.
B,C. Photomicrograph (hematoxylin-eosin stain) of the cut surface along the broken line in Fig. A is shown in Fig. B,C. Hemorrhage in the wall (B, yellow arrow) of the tube is observed. Villi (C, arrow) invading the tubal wall is demonstrated.")
, and fat-suppressed T1-weighted (B) MRI. A GS-like structure is typically a cystic lesion with relatively thick wall.
On T2-weighted MRI, its wall shows high intensity (A, red arrow) and contains distinct low intensity area (A, yellow arrow). On fat-suppressed T1-weighted MRI, part of the wall shows high intensity (B, arrow).
C,D. Photomicrograph (hematoxylin-eosin stain) of the wall of the GS-like structure demonstrates edematous change (C, circle) and hemorrhagic change (D, arrow) of the wall.
These findings can explain the MRI findings.
This is one of the useful findings to differentiate a GS-like structure from a corpus luteum cyst.")
 with its wall enhanced intensely. Note intensely enhanced papillary projection in the fallopian tube (B, red arrow).
D,E,F Axial T2-weighted MRI demonstrate contents of dilated fallopian tube (D,E,F, yellow arrows), which show heterogeneously low signal suggesting hematoma.")
. Ut: Uterus")
 and magnification of a corpus luteum cyst (B) show cystic lesion (A, arrow) with thickened wall in the right ovary. Around the cystic lesion, several small cysts (B, arrow) representing follicular cysts are found, and this finding suggests that the lesion is a corpus luteum cyst.
C. Axial gadolinium-enhanced fat-suppressed T1-weighted MRI shows the corpus luteum cyst (arrow) with its wall strongly enhanced, and this finding is identical with a GS-like structure.")
 was found at the periphery of the right ovary.
B. Macroscopic photograph shows the cystic lesion with whitish or slightly yellowish wall, which is compatible with a corpus luteum cyst.
C,D. Photomicrograph (hematoxylin-eosin stain) of the corpus luteum cyst.
Figure D is the magnification of the wall. Most of the wall consists of granulosa lutein cells with clear cytoplasm.
At the periphery of the wall, Theca cells form dendritic projection. Granulosa lutein cells (E, arrow) contain fat in their cytoplasm, so corpus luteum cysts usually have macroscopically yellowish appearance.")
 and fat-suppressed T1-weighted (B) MRI show hematoma (A,B, arrow) at the right adnexa.
C. Coronal T2-weighted MRI (C) reveals small cysts (C, arrow) around the hematoma. This finding suggests the hematoma is located in the ovary.")
 shows granulosa lutein cells in the wall, and no evidence of ectopic pregnancy.")
, and the junctional zone is uninterrupted.
The myometrium embodies the GS-like structure (A, yellow arrow), this finding facilitates differentiating from ectopic pregnancy within the tubal isthmus.")
 and isthmus of fallopian tube (yellow arrow).
B. Photomicrograph (hematoxylin-eosin stain) shows villous tissue (arrow) invading myometrium. Around the implantation site, massive hemorrhage is found.
C,D. Intraoperative photographs of left interstitial pregnancy (another case) show a dark red mass at the interstitial portion of the fallopian tube (C, arrow). Left ovary is identified (D, arrow).")
 and coronal (B) T2-weighted MRI show a GS-like structure (arrows) at the right cornus and it is located inside the junctional zone.")
 demonstrate marked vascurality of the GS-like structure (arrows).")
 and villous tissue (yellow arrow).
B. Photomicrograph (hematoxylin-eosin stain) shows villous tissue (yellow arrow) and the epithelium of the cervix (red arrow).")
, just in touch with right ovary (yellow arrow).")
 of ovarian pregnancy.
Inside the ovarian stroma, hemorrhagic villi and trophoblast cells are identified. No evidence of tubal pregnancy is found. Follicle of the ovary (A, arrow) is shown.")
 at the cesarean scar. The uterine myometrium of the implantation site is markedly thin.
B. Sagittal gadolinium-enhanced fat-suppressed T1-weighted MRI shows the enhanced GS-like structure (arrow).")
 at 6 weeks’ gestation.
A. Sagittal T2-weighted MRI shows a GS-like structure (arrow) in the omentum.
B,C. Axial T2-weighted (B) and gadolinium-enhanced fat-suppressed T1-weighted MRI show the GS-like structure (B,C, arrow) and hemoperitoneum.")
 was identified in the omentum, and resected.
B,C. Photomicrograph (hematoxylin-eosin stain) of the pregnancy.
Trophoblast cells (yellow arrow) invading omentum (red arrow) are found, which indicates this is the implantation site. Extensive hematoma around the lesion is also found.")
 of 6 weeks’ gestation.
A. Sagittal T2-weighted MRI shows hematoma (arrow) in the vesicouterine pouch.
B,C. Axial T2-weighted (B) and gadolinium-enhanced fat-suppressed T1-weighted (C) MRI show a GS-like structure (arrows) inside the hematoma in the vesicouterine pouch.")
.
A. Intraoperative photograph shows a mass covered with hematoma (arrow) at the vesicouterine pouch. Ut: uterus, Ov: ovary
B. Magnification of the implantation site. Rl: round ligament
C. Photomicrograph (hematoxylin-eosin stain) demonstrates villous tissue (arrow).")