ECR 2014 / C-1524
Imaging of the normal male urethra from the neonate to the elder: radiologic anatomy in fluoroscopic urethrography.
This poster is published under an open license. Please read the disclaimer for further details.
Congress:
ECR 2014
Poster Number:
C-1524
Type:
Educational Exhibit
Keywords:
Education and training, Normal variants, Cystography / Uretrography, Fluoroscopy, Genital / Reproductive system male, Anatomy
Authors:
A. Charsoula, D. Katsiba, C. Kaitartzis, A. Papadimitriou, C. NALMPANTIDOU, I. Torounidis, D. Rafailidis, M. Arvaniti; Thessaloniki/GR
DOI:
10.1594/ecr2014/C-1524

Fig. 2:
The location of the internal urethral sphincter in association with the...

Fig. 3:
a. RUG: Posterior urethra may not be shown at all even in normal subjects....

Fig. 4:
In urethrography male urethra is shaped like a horizontally inverted “S”.

Fig. 5:
The prostatic urethra begins at the vesical neck, courses through the prostatic...

Fig. 6:
The verumontanum produces an oval filling defect at the middle of the posterior...

Fig. 7:
The intermuscular incisura creates an indentation at the anterior wall of the...

Fig. 8:
The plicae collicularis appear as thin, non-obstructing indentations caudally...

Fig. 9:
The prostatic utricle may fill with contrast during urethrography, creating a...

Fig. 10:
Beginning from the apex of the prostate gland, the membranous urethra traverses...
 and the conical end of the bulbar urethra (distally-red arrow).")
Fig. 11:
The membranous urethra lies specifically between two radiologic landmarks: the...
 at the level of the external urethral sphincter. The penoscrotal junction can be identified by a mild angulation caused by the suspensory ligament (red arrow). In VUG studies (fig 12c) the bulbar urethra has a less conical appearance and the anterior urethral lumen appears narrower than in RUG studies.")
Fig. 12:
RUG shows the anterior urethra as a long, wide lumen that tapers smoothly to a...
 located at the proximal bulbous urethra and the fossa navicularis (red arrow) at the distal penile urethra within the glans penis.")
Fig. 13:
The “sump” of the bulbous urethra (yellow arrow) located at the proximal...

Fig. 14:
The bulbospongiosus muscle may produce a false image of stenosis of the whole...

Fig. 15:
The constrictor nudae muscle, creates a mild indentation at the bulbous...

Fig. 16:
When there is forceful injection of contrast material in RUG or more commonly ...

Fig. 17:
During VUG in uncircumcised patients, contrast material may accumulate between...
: indentations from internal urethral sphincter in children.")
Fig. 18:
Urethrograms in boys and adults do not differ as far as radiologic anatomy is...

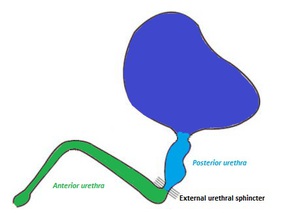
Fig. 19:
Anatomy of the male urethra.