MATERIALS,
METHODS AND RESULTS: (Fig 3&4)
We retrospectively reviewed cases of non-traumatic cerebral hemorrhage from the PACS from July 2010-June 2013 (n = 65; 33 women,
32 men,
median age at diagnosis 65 years [range 18-95 years].
Inclusion criteria included only those patients with proven etiologies for the hemorrhage.
We evaluated the clinical presentation and etiology of the hemorrhage based on multimodality imaging findings.
Clinical symptoms:
Sudden onset focal neurologic deficit was the most common presentation (n=40).
In 15 cases headache with nausea and vomiting was the first clinical presentation and in 8 cases,
alteration in the level of consciousness was noted.
2 patients presented with seizures.
Bassed on Etiology:
We categorised intracranial hemorrhage based on etiology of the bleed.
Hypertensive Bleed (n=20; 30.7%),
Cerebral Amyloid Angiopathy (n =14; 21.5%),
Arteriovenous Malformation (n=11; 16.9),
Neoplasm (n=8; 12.3%),
Aneurysmal bleed (n=4,
6.15%).
Hemorrhagic Infarct (n=3; 4.6%),
Venous Sinus Thrombosis (n=2; 3.07%) and Others (n=3; 4.6%)
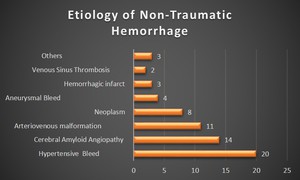
Fig. 3: Cluster bar chart comparing the number of patients, based on the various etiologies causing non-traumatic parenchymal bleed
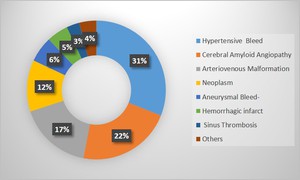
Fig. 4: Doughnut demonstrating incidence of various etiologies of non-traumatic cerebral hemorrhage
FINDINGS:
A) Hypertensive Hemorrhage:
•Leading cause in adults.
•Pathophysiology:(Fig 5)
- Ruptured micro-aneurysms (Charcot-Bouchard) of deep perforating branches of MCA & basilar artery,
secondary to reactive hyperplasia of smooth muscle cells of cerebral arterioles and resultant collagen deposition.
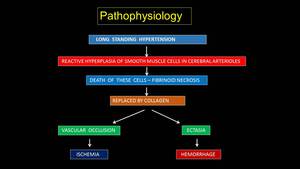
Fig. 5: Pathophysiology of Hypertensive bleed
•Sites:- (Fig 6 & 7)
- Putamen-external capsule,
thalamus,
pons,
cerebellum,
lobar white matter +/- intraventricular extension
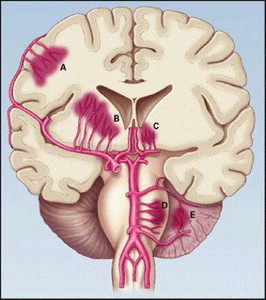
Fig. 6: Most Common Sites and Sources of Intracerebral Hemorrhage
References: The New England Journal of Medicine
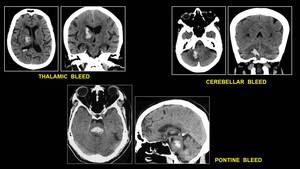
Fig. 7: Multiplanar CT Scan of common sites of Hypertensive Bleed
•Other findings:
- Diffuse microvascular ischemic changes in white matter
- Lacunar infarcts
- Microbleeds
•DD:
- Drug abuse related hemorrhage – younger patient
•Hematoma expansion:
- More than 1/3rd in upto 38% of patients
- Seen as focal contrast extravasation
- Poor outcome
B) Cerebral Amyloid Angiopathy: (Fig 8)
•Deposition of β-amyloid protein in wall of small & medium sized blood vessels of the cerebral cortex and leptomeninges.
•2 types
-Sporadic
-Inherited - Less common,
earlier onset,
associated with dementia
•15-20% of all ICHs in normotensive patients above 55yrs
•Location:
-Lobar hemorrhage,
cortical or subcortical without another cause
•Other findings:
- Multiple microbleeds-peripheral subcortical,
more in parietal lobes and cerebellum
- Spares basal ganglia and brainstem
- Associated superficial hemosiderosis
- White matter ischemia
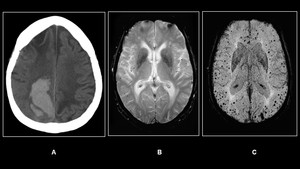
Fig. 8: (A)Non-enhanced Axial CT in an elderly patient shows an acute right lobar hematoma(B)GRE &(C)SWI shows multiple micro bleeds.
C) Hemorrhagic Ischemic Stroke: (Fig 9)
•Secondary hemorrhage in ischemic cerebral infarction
•Pathology:
- Reperfusion of ischemically damaged vascular endothelium with
extravasation of blood.
- Embolic more than thrombotic occlusion
- Petechial hemorrhage/Parenchymal hematoma in the infarcted
brain parenchyma on imaging studies.
•Location: Predilection for basal ganglia and cortex
•Incidence: 2- 40%,
symptomatic – 6-12%
Outcome prediction: Parenchymal hematoma more than one third of ischemic area – Poor prognosis
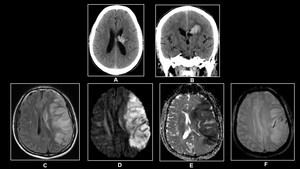
Fig. 9: (A)&(B)Non-enhanced Axial CT demonstrates hemorrhage in left corona radiata infarct.(C) FLAIR,(D)DWI,(E)ADC &(F)GRE demonstrates hemorrhagic left MCA infarct in a 70 year old male with dense right hemiplegia
D) Aneurysmal Subarachnoid Hemorrhage: (Fig 10 & 11)
•5% of Stroke cases,
Mortality – 12-66%
•Risk Factors:
- Hypertension,
smoking,
female gender
•Clinical Features:
“Worst headache of life”
•Diagnosis:
- Imaging,
lumbar puncture
CT Findings:
- Increased density in basal cisterns
- Parenchymal hematoma
- Mass-like appearance with large filling defect and calcification
- CTA: rounded contrast filled outpouching of vessel wall
- Common locations: ACom,
Pcom,
MCA trifurcation,
Basilar tip and
PICA
CT Findings:
“Fisher Grade”
1: No blood detected
2: Diffuse thin (< 1 mm) Subarachnoid Hemorrhage (SAH) with no clots
3: Localised clots and / or layers of blood > 1 mm in thickness
4: Intracerebral or intraventricular blood (+/- SAH)
•MRI/MRA:
- Increased signal of CSF on FLAIR images
- Chronic hemorrhage – Superficial siderosis
•DSA:
- Negative CTA
- Pre-operative evaluation of complex aneurysms
- Detect additional asymptomatic aneurysms
- Intra-arterial treatment of vasospasm
•Transcranial Doppler:
- To detect vasospasm after SAH
- Mean cerebral blood flow velocity (MCBFV) of >120 cm/sec
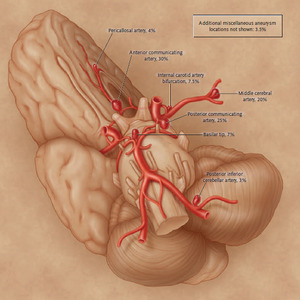
Fig. 10: Intracranial Vasculature showing most frequent locations of Intracranial Aneurysms.
References: Jonathan L.et.al, Cerebral Aneurysms.N Engl J Med 2006; 355:928-939
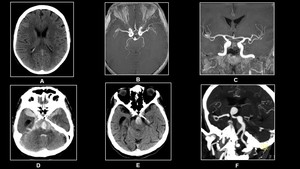
Fig. 11: 55 year old female with severe headache.(A)Non-enhanced CT,(B)and(C) 3D TOF reveals Aneurysms at bifurcation of both MCA's with subarachnoid hemorrhage.
80 year old unconscious male.(D)&(E)Non-enhanced CT and(F) CT Angiography reveals tip of basilar aneurysm with subarachnoid hemorrhage
E) Vascular Malformations:
•20% cases of spontaneous ICH
•Leading cause of ICH in young adults.
•Types:
a) Arteriovenous malformations (AVM's)
b) Dural arteriovenous fistulas (DAVF's)
c) Cavernous malformations
d) Developmental venous anomalies (DVA's)
a) AV Malformations: (Fig 12)
- Developmental lesion in the brain parenchyma
- Abnormal connection between pial arteries & veins with no
intervening capillary bed
- Site of anomalous communication- central nidus with variable size
•CT findings:
- Intracranial hemorrhage
- Enlarged serpiginous dense feeding arteries &/or veins
- Encephalomalacia
- Calcification
- Direct visualization of vessels on contrast enhanced CT
•MRI/MRA:
- Abnormal vessels visualized
•DSA:
- For small occult AVMs not appreciated on CT & MRI for complete
characterization
- Therapeutic intervention
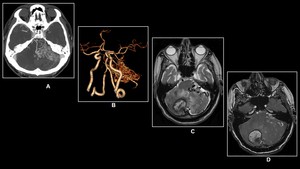
Fig. 12: 38 year old male with severe vertigo and loss of balance
(A) CT angiography and (B) Volume Rendering Technique (VRT)reveals tangle of vessels in the posterior fossa which demonstrates nidus of feeding arteries and draining veins.(C) Axial T2W MRI and (D)3D TOF image reveals right cerebellar hemorrhage with associated AVM.
b) Dural AV Fistulas: (Fig 13)
- Arteriovenous shunting within dura
- Abnormal direct connection between a meningeal artery & vein or
dural venous sinus
•Etiology:
- Acquired & idiopathic
- H/o Dural venous sinus thrombosis,
surgery or trauma
- Rarely congenital
•Common location: cavernous sinus,
posterior fossa
•Non-contast enhanced CT:
- Normal
- Hemorrhage
- Hydrocephalus
- Dense vessels seen
•Contrast-enhanced CT:
- Abnormal enlarged tortuous feeding arteries,
draining veins &
occluded dural sinuses
•MRI,
MRA show similar findings
•Contrast enhanced MRA – Useful to identify fistulous communication
•DSA:
- For occult lesions on CT/MRI
- Detailed assessment
- Endovascular treatment
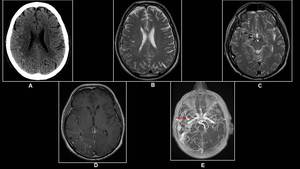
Fig. 13: 20 year old male with occasional headaches.
(A) Non-enhanced CT, (B)&(C) Axial T2W,(D)Post- Contrast T1 Axial &(E) 3D TOF images reveal prominent and tortuous right middle meningeal artery(arrow)with cluster of flow voids in the right frontoparietal lobe appreciated as hyper dense foci on the Non-enhanced CT.
c) Cavernous Malformations: (Fig 14)
•Incidence: 0.2 – 0.4% of population
•Pathology:
- Low flow vascular hamartoma
- Closely apposed endothelial-lined blood vessels without intervening
brain tissue
- Anywhere in the brain
- Solitary or Multiple(genetic syndrome)
- Associated with DVA
•Clinical Features :
- Headache,
seizures,
acute ICH or incidental finding
•CT SCAN:
- Often not well visualized
- Round-to-oval shaped area of subtle hyper density – blood
products & calcification
- Acute hemorrhage
•MRI:
- Mixed Signal intensity core on T1 & T2W (“popcorn” like
appearance) with low signal peripheral rim on GRE
- Post contrast: To demonstrate associated DVA,
if any
• DSA:
- Occult,
no role.
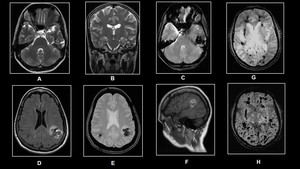
Fig. 14: (A)-(C)Illustrates left temporal lobe cavernous malformation on the T2W and GRE sequences.(D)-(F)demonstrates intraparenchymal bleed from cavernous malformation.(G)and(H)GRE and SWI respectively reveals that cavernous malformation are better demonstrated on the SWI sequence.
F) Venous Thrombosis:(Fig 15)
- 1-2% of stroke in adults
- Common in younger age group
•Pathology:
- Thrombosis causing venous hypertension resulting in venous
ischemia,
infarction and hemorrhage
•Location:
- Posterior temporal lobes
- Parasagittal frontal & parietal lobes
- Both thalami
•CT SCAN:
- Edema & hemorrhage,
if venous infarct
- Hyperdensity in sinuses and cortical veins (“cord sign”)
- Filling defect or lack of opacification in a vein or sinus on CECT
(“Empty delta sign”)
•MRI:
- Edema & hemorrhage (more sensitive than CT),
GRE sequence
- Variable restricted diffusion•Loss of flow void signal in dural sinuses
- Abnormal signal intensity in cortical vein or sinuses
- MRV – Absent flow
- Postcontrast– “empty delta” sign
•DSA:
- No role in diagnosis
- Administration of intravenous thrombolytic agents
- For mechanical clot lysis
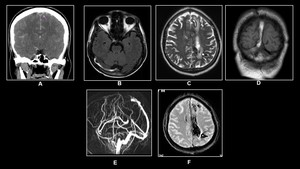
Fig. 15: 25 year old female on OC pills with severe headache and vomiting
(A)Non-enhanced CT,(B)&( D)T1W Axial and Coronal,(C)T2W Axial,(E)MR Venography and(F)GRE reveal Hemorrhagic Venous Sinus Thrombosis.
G) Hemorrhage in Neoplasms:(Fig 16 & 17)
•Primary or Metastatic tumors
- Primary- GBM,
Pituitary adenoma
- Metastasis – Choriocarcinoma,
melanoma,
thyroid Ca,
renal cell Ca.
Lung & breast more common.
•CT Scan:
- Hemorrhage
- Disproportionate edema
- Heterogeneous hematoma
•MRI:
- Extremely heterogeneous–tumor,
necrotic tissue,
blood products
- Debris-fluid level
- Mixed enhancing and non-enhancing areas
- Incomplete peripheral hemosiderin rim
- Delayed evolution of blood breakdown products
- Persistent edema and mass effect
- Presence of other enhancing lesions (Metastasis)
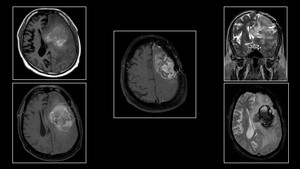
Fig. 16: Hemorrhage in Glioblastoma(GBM)in a 78 year old male with seizures.
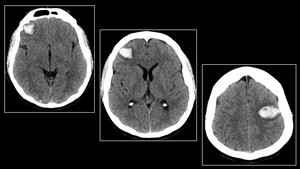
Fig. 17: Hemorrhagic metastasis from extra gonadal choriocarcinoma
H) Vasculitis,
Vasculopathy,
Vasospasm
•Vasculitis: (Fig 18)
- Multifocal areas of ischemia & hemorrhage in deep grey matter & subcortical white matter.
DSA useful
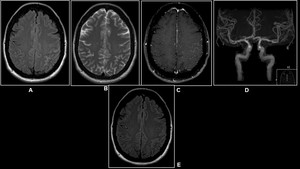
Fig. 18: 45 year old female with confusion.
(A)FLAIR,(B)T2W Axial &(C)Post-Contrast T1W demonstrates subarachnoid hemorrhage in the left parietal lobe.(D)3D TOF reveals irregularity of both MCA.(E) FLAIR Axial shows complete resolution after 6 months.
•Vasculopathy:
- Ischemia more common than hemorrhage eg; Moya Moya disease.
Rupture of fragile collaterals & aneurysms
•Reversible Cerebral Vasoconstriction Syndrome (RCVS): (Fig 19)
- Prolonged but reversible.
Ischemia & hemorrhage.
- CTA/MRA/DSA: Diffuse vascular irregularity
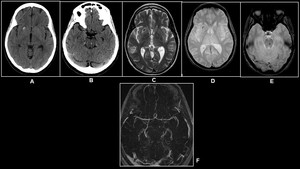
Fig. 19: Middle age woman with SLE
(A)&(B)Non-enhanced CT,(C)T2W Axial &(D)and(E)GRE reveal hemorrhagic foci in the right putamen and pons.(D)3D TOF reveals irregularity and beaded appearance of M2 segment of left MCA.
I) OTHER MISCELLANEOUS CAUSES
|
I) Subdural hematoma
( spontaneous)
•Benign intracranial hypotension
•Hemorrhagic dural metastases
•Clotting disorders
•Ruptured aneurysms
|
II)Other Causes of ICH
•Anticoagulant therapy
•Clotting factor deficiency
•Hepatic dysfunction
•Metabolic disorders
•Viral encephalitis
•Non-aneurysmal SAH
|
a) Spontaneous Intracranial hypotension: (Fig 20)
• Patients usually present with postural headache
• Etiologies include trauma to the paranasal sinuses or spinal
intervention.
Most cases however are idiopathic
• Subdural hemorrhage occurs due to stretching and eventually
tearing of the bridging cortical veins by the downward displacement
of the brain rather than vascular engorgement of the dura.
• MRI
- Bilateral subdural collections/bleed with diffuse pachymeningeal
enhancement.
- Sagging of the brainstem with tonsillar herniation,
- Crowding and effacement of the suprasellar cisterns with
reduction in the mamillo-pontine distance
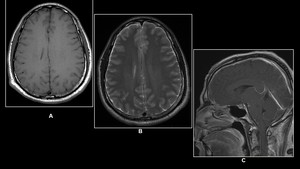
Fig. 20: 37 year old male with postural headache
(A)T1W (B) T2W Axial &( C)Post- Contrast Sagittal T1W MRI reveals minimal bilateral subdural collection with pachymeningeal enhancement and sagging of the brainstem
b) Anti-coagulant therapy:
- Similar to primary hemorrhage
- Location: Supratentorial and Intraparenchymal common
- Fluid-fluid levels
- Multiple large hemorrhages
- Significant mass effect
c)Perimesencephalic non-aneurysmal subarachnoid hemorrhage
(Fig 21)
- Benign subarachnoid hemorrhage confined to the
perimesencephalic and prepontine cisterns.
- Patients usually present with mild to moderate headache,
rarely
thunderclap headache.
- It is self-limited,
rarely cause vasospasm and probably secondary to
venous hemorrhage.
- CTA needs to be performed to rule out basilar tip aneurysm
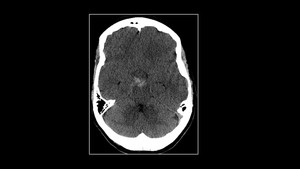
Fig. 21: 35 year old female with thunderclap headache. Non-contrast Axial CT reveals blood density in the perimesencephalic cistern. CT Angiography done was unremarkable.
IMAGING APPROACH TO NON-TRAUMATIC INTRACEREBRAL HEMORRHAGE ( Fig 22)
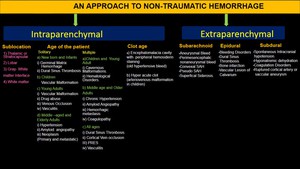
Fig. 22: Imaging Approach to non-traumatic intracerebral bleed






Non-enhanced Axial CT in an elderly patient shows an acute right lobar hematoma(B)GRE &(C)SWI shows multiple micro bleeds.")
&(B)Non-enhanced Axial CT demonstrates hemorrhage in left corona radiata infarct.(C) FLAIR,(D)DWI,(E)ADC &(F)GRE demonstrates hemorrhagic left MCA infarct in a 70 year old male with dense right hemiplegia")

Non-enhanced CT,(B)and(C) 3D TOF reveals Aneurysms at bifurcation of both MCA's with subarachnoid hemorrhage.
80 year old unconscious male.(D)&(E)Non-enhanced CT and(F) CT Angiography reveals tip of basilar aneurysm with subarachnoid hemorrhage")
 CT angiography and (B) Volume Rendering Technique (VRT)reveals tangle of vessels in the posterior fossa which demonstrates nidus of feeding arteries and draining veins.(C) Axial T2W MRI and (D)3D TOF image reveals right cerebellar hemorrhage with associated AVM.")
 Non-enhanced CT, (B)&(C) Axial T2W,(D)Post- Contrast T1 Axial &(E) 3D TOF images reveal prominent and tortuous right middle meningeal artery(arrow)with cluster of flow voids in the right frontoparietal lobe appreciated as hyper dense foci on the Non-enhanced CT.")
-(C)Illustrates left temporal lobe cavernous malformation on the T2W and GRE sequences.(D)-(F)demonstrates intraparenchymal bleed from cavernous malformation.(G)and(H)GRE and SWI respectively reveals that cavernous malformation are better demonstrated on the SWI sequence.")
Non-enhanced CT,(B)&( D)T1W Axial and Coronal,(C)T2W Axial,(E)MR Venography and(F)GRE reveal Hemorrhagic Venous Sinus Thrombosis.")
in a 78 year old male with seizures.")

FLAIR,(B)T2W Axial &(C)Post-Contrast T1W demonstrates subarachnoid hemorrhage in the left parietal lobe.(D)3D TOF reveals irregularity of both MCA.(E) FLAIR Axial shows complete resolution after 6 months.")
&(B)Non-enhanced CT,(C)T2W Axial &(D)and(E)GRE reveal hemorrhagic foci in the right putamen and pons.(D)3D TOF reveals irregularity and beaded appearance of M2 segment of left MCA.")
T1W (B) T2W Axial &( C)Post- Contrast Sagittal T1W MRI reveals minimal bilateral subdural collection with pachymeningeal enhancement and sagging of the brainstem")

