FREQUENCY OF ANKLE INJURIES
Ankle injuries are one of the most common articular injuries in the body with an estimated incidence rate of 2.15 per 1000 person-years.
The peak incidence of ankle injuries occurre between fifteen and nineteen years of age (7.2 per 1000 person-years).
Supination injuries predominate,
causing more trauma at the lateral side.
85% of the injuries are "sprains",
while 15% is more complex.
Nearly half of all ankle sprains occur during athletic activity,
such as soccer.
I.
OSTEOARTICULAR ANATOMY OF THE ANKLE
I.
A.
Bony anatomy
The ankle is composed of three main articulations: the distal tibiofibular (syndesmotic) joint,
the talocrural (ankle) joint and the subtalar (talocalcaneal) joint (Fig. 1).
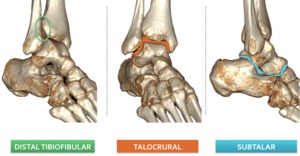
Fig. 1: 3D CT illustrations demonstrating the three articulations of the ankle.
Looking at the shape of the ankle bones,
one might compare the ankle joint with a Mortise-Tenon joint,
which is a very stable articulation (Fig. 2).
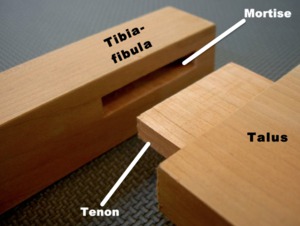
Fig. 2: Comparison Mortise and Tenon joint to tibiofibular articulation.
However,
there are some major differences in the talocrural joint.
First,
the articular surface of the talus is shaped like a cone rather than a rectangle () ,
with the anterior part being wider than the posterior part.
Second,
the articular sides of medial and lateral malleoli are not of the same length (Fig. 3).
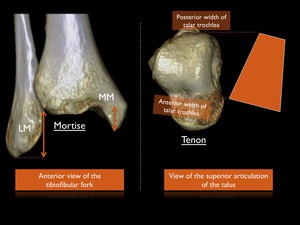
Fig. 3: 3D CT illustrations pointing out the differences of the ankle joint with a mortise and tenon.
Therefore the tibiofibular joint relies on ligaments for its stability.
These ligaments will be discussed in greater detail further on in this exhibit.
The subtalar joint (Fig. 4) exists of an anterior and posterior part.
The anterior part (also called talocalcaneonavicular joint) is made up by the anterior and middle facets of the talus and calcaneus,
as well as the talonavicular joint.
The posterior part is formed by the talar and calcaneal posterior facets.
In a normal situation these two joints do not communicate: they are separated by ligaments within the tarsal sinus and canal.
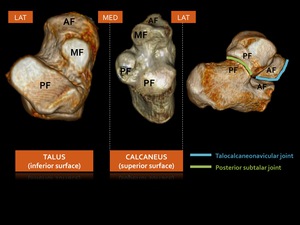
Fig. 4: 3D CT illustrations showing the corresponding facets at the undersurface of the talus and the superior surface of the calcaneus: subtalar joint. AF = anterior facet. MF = middle facet. PF = posterior facet.
I.
B.
Lateral ligamentous complex
The lateral ligamentous complex consists of three ligaments between the fibula and talus or calcaneus: anterior talofibular ligament (ATaFL),
calcaneofibular ligament (CFL) and posterior talofibular ligament (PTaFL).
Most injuries of this lateral collateral complex are usually secondary to inversion trauma with supination of the foot combined with ankle plantar flexion.
The damage caused by an inversion trauma depends on the velocity of the impact,
weight of the individual,
age of the patient and weaknesses generated by previous injuries.
In approximately 70% of all ankle ligament ruptures,
the ATaFL tears alone.
Combined ruptures of the ATaFL and the CFL occures in 20% of cases.
Isolated ruptures of the CFL are rare ,
as well as injury to the PTaFL.
The latter occurs with frank dislocation of the ankle.
I.
B.1.
Anterior talofibular ligament
The ATaFL is the first and most common lateral ligament to rupture.
This flat ligament runs from the anterior margin of the lateral malleolus anteromedially towards its insertion on the anterior border of the lateral articular surface of the talus (lateral body-neck junction).
It is a capsular structure,
explaining the presence of intracapsular ossicles after avulsion,
which may simulate true intra-articular bodies.
The ATaFL typically exists of two separate bands (superior and inferior),
with a common origin on the fibular side,
a bifid talar insertion and an overall width of 6 - 10mm (Fig. 5).The length of an intact superior ATaFL is estimated to 20 mm and that of the inferior ATaFL is estimated to 17 mm.
These bands may tear partially or completely.
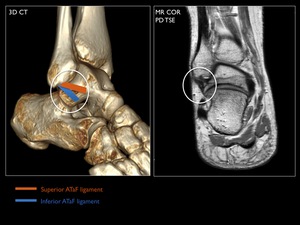
Fig. 5: 3D CT illustration with MR (coronal oblique) correlation of the superior and inferior ATaFL.
The distance between the superior and inferior ATaFL footprints on the talus,
measured center to center,
is estimated to 12 mm.
Variants with a single and with three bands are described.
The vascular branches of the anterior fibular artery runs between the two bands.
The double bundle creates a biomechanical advantage: the superior ATaFL will be taut in plantar flexion and the inferior ATaFL will be taut in dorsiflexion (Fig. 12).
Since the superior ATaFL restricts inversion in plantar flexion - being the most common position of the foot at the time of injury - it may be the more important of the 2 bundles.
Both bands of the ATaFL play an important role in limiting anterior displacement of the talus,
especially with plantar flexion.
It also limits internal rotation of the talus and external rotation of the fibula.
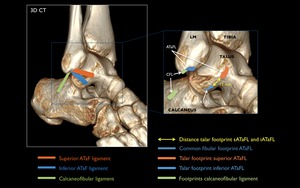
Fig. 6: 3D CT with schematic representation of the footprints of the ATaF and CF ligaments.
I.B.2.
Calcaneofibular ligament
The CFL originates from the anterior part of the lateral malleolus,
positioned just below the inferior band of the ATaFL (Fig. 5).
Frequently,
fibers connecting both ligaments can be observed.
In the neutral ankle position,
the CFL runs obliquely down - and backwards to insert to a small tubercle on the posterior aspect of the lateral calcaneal surface.
This ligament measures about 20mm in length and is superficially crossed by the peroneal tendons and sheaths,
possibly leaving a concavity over the ligament.
It is intimate with the lateral talocalcaneal ligament,
which can be mistaken for an intact CFL when the CFL is ruptured.
The CFL is the only extra-capsular ligament,
related to two joints (ankle and posterior subtalar joint).
In contrast,
the ATaFL and the PTaFL are ligaments related to the ankle joint only.
This is important to realize,
since the CFL is not only a stabilizer of the ankle joint,
but also stabilizes the posterior subtalar joint.
Usually,
in inversion trauma at the ankle joint,
the injury begins at the ATaFL and proceeds to the CFL.
Injuries of the posterior subtalar joint may show isolated disruption of the CFL.
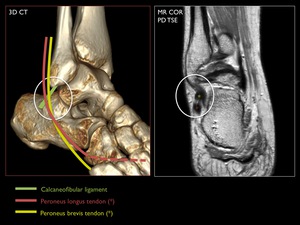
Fig. 7: 3D CT illustration with MR correlation of the calcaneofibular ligament and the crossing peroneal tendons.
The CFL becomes horizontal during plantar flexion and vertical in dorsal flexion,
remaining taut in both positions (Fig. 12).
A valgus or varus position of the talus considerably changes the angle formed by the CFL and the longitudinal axis of the fibula.
The ligament relaxes in the valgus position and tenses in the varus position,
explaining the potential for injury in abscence of dorsiflexion / plantar flexion movement in the ankle.
The CFL limits anterior translation and internal rotation of the talus,
as well as external rotation of the fibula with dorsiflexion.
I.B.3.
Posterior talofibular ligament
The PTaFL is a very strong capsular ligament which runs almost horizontally from the malleolar fossa (medial surface of the lateral malleolus) to the posterolateral talus .
In the neutral ankle position and in plantar flexion,
the ligament is relaxed,
while in dorsiflexion,
the ligament is taut (Fig. 12).
The insertion on the posterolateral talus may vary due to the multifascicular aspect of this ligament: insertion is possible on the posterior surface of the talus,
the lateral talar process or os trigonum,
if present.
Some fibers may contribute to the floor of the flexor hallucis longus tendon tunnel.
Moreover,
a group of fibers fuse with the posterior intermalleolar ligament,
which is involved in the posterolateral impingement of the ankle.
As mentioned higher,
the PTaFL is the least susceptible to injury,
except in major ankle dislocations.
Its function is to limit posterior translation and external rotation of the talus,
as well as internal rotation of the fibula.
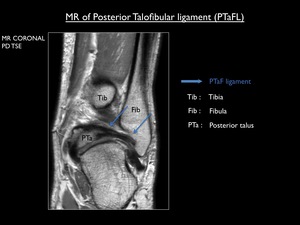
Fig. 8: Coronal proton-density MR image demonstrating the posterior talofibular ligament
I.C.
Syndesmotic (tibiofibular) ligament complex
The syndesmotic ligaments ensure the stability of the distal tibiofibular joint by resisting axial,
rotational and translational forces attempting to separate the tibia and fibula.
This complex consists of four ligaments : anterior tibiofibular ligament (ATiFL),
interosseous ligament (IOL),
(superficial) posterior tibiofibular ligament (PTiFL),
transverse inferior tibiofibular ligament (TITFL).
A fifth ligament (Bassett's ligament) may also occur.
I.C.1.
Anterior tibiofibular ligament
The ATiFL extends between the anterior border of the lateral malleolus and anterolateral tubercle of the distal tibia.
It consists of two or three bands (sometimes four),
with fibers directed upward and medially.
Multiple branches from the peroneal artery run in between the different bands.
The lowest band can be large and oriented more horizontal,
potentially causing some confusion with the ATaFL or with a possible Bassett's ligament.
An injury to the ATiFL will always be associated to partial or complete tearing of the interosseous ligament.
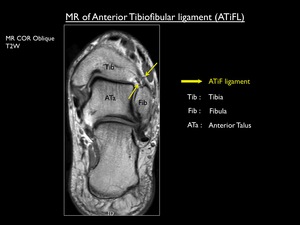
Fig. 9: T2 weighted MR image showing two bands of the anterior tibiofibular ligament (AiTFL).
I.C.2.
Interosseous ligament
The IOL presents as a dense mass of short fibers,
running obliquely from proximal tibial to more inferiorly fibular and spanning the tibia to the fibula.
Actually it is a distal continuation of the interosseous membrane,
forming a roof over the syndesmotic recess of the ankle joint.
I.C.3.
Posterior tibiofibular ligament
The PTiFL is formed by a superficial and a deep portion.
The superficial PTiFL is a triangular structure (wider on the fibular side),
which finds its origin at the posterior border of the lateral malleolus and runs proximally and medially to insert on the posterior tibial tubercle.
It is intimate with the posterior part of the interosseous ligament.
The deep portion (also known as the transverse inferior tibiofibular ligament) forms a true labrum,
and runs from the proximal malleolar fossa to the posterior tibial border.
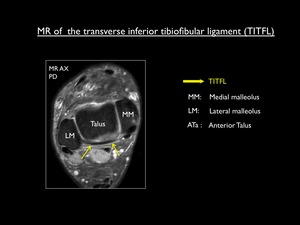
Fig. 10: Axial proton density MR image showing the transverse inferior tibiofibular ligament.
I.C.4.
Bassett's ligament (= accessory ATiFL)
Bassett's ligament is a controversial structure : Some think it is a fascicle of the ATiFL,
others think it is an anomalous ligament.
It is defined as a thick ligament below the usual region of the ATaFL,
curving over the lateral corner of the talar dome.
Clinically it may cause anterolateral impingement of the ankle.
I.D.
Medial ligamentous complex (deltoid ligament)
There is considerable disagreement in the literature on this ligament.
Most authors on the deltoid ligament agree that it is composed of a superficial and deep portion.
The description of what make up these portions vary widely.
Based upon most descriptions,
the deep portion of the deltoid ligament is composed of ligaments located between tibia and talus: the deep anterior and posterior tibiotalar ligament.
The deep posterior tibiotalar ligament is the strongest and most important ligament of the deep portion.
It runs from the posterior tibial colliculus/intercollicular groove to the medial side of the talus (concave insertion).
The deep anterior tibiotalar ligament is less important and may even be absent.
It runs from the anterior colliculus to the medial side of the talus.
The superficial deltoid portion is a broad structure,
originating mainly to the anterior tibial colliculus.
It consists of the tibionavicular,
tibiospring, tibiocalcaneal and superficial posterior tibiotalar ligaments.
| Superficial portion |
Deep portion |
| Tibionavicular ligament* |
Deep posterior tibiotalar ligament* |
| Tibiospring ligament* |
Deep anterior tibiotalar ligament |
| Tibiocalcaneal ligament |
|
| Superficial posterior tibiotalar ligament |
|
Table 1: Components of the medial ligamentous complex (*constant ligaments)
The function of the deltoid ligament is to provide stability of the medial ankle joint.
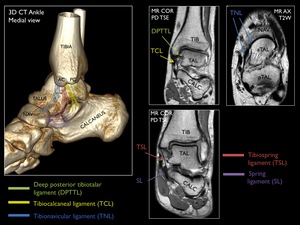
Fig. 11: 3D CT of the ankle from a medial view with a schematic representation of the main components of the deltoid ligament and the spring ligament.
II.
BIOMECHANICS
The ankle joint is a hinge type,
allowing mainly plantar flexion of 20-50°,
and dorsiflexion of 10-30°.
Other movements in the ankle joint are minimal abduction/adduction and internal/external rotation.
Complex movements take place at the posterior subtalar joint,
due to obliquely (posteromedial to anterolateral) oriented facets.
If the posterior facets were oriented in a mediolateral plane,
plantar flexion and dorsiflexion would be the only motion.
If the posterior facets were oriented in an anteroposterior plane,
the only motion would be supination and pronation.
In reality the motion is complex and described as supination-plantar flexion and pronation-dorsiflexion.
Since the talus is cone-shaped (see higher - Fig. 3) with a wider anterior portion,
the distal tibiofibular joint has to accomodate a larger talar surface in dorsiflexion and has to close the joint in plantar flexion.
With dorsiflexion,
the ankle joint has to widen maximally to fit the talus.
This will be accomplished by adapting the width of the syndesmotic space,
through slight ascending and external rotation of the fibula.
The talus also demonstrates slight external rotation.
The ATaFL becomes relaxed and more horizontal,
while the CFL and PTaFL become tight and more vertical.
This allows the talus to move dorsally.
The main stabilizer in this position is the CFL.
Dorsiflexion is the most stable position of the ankle,
since in this situation the joint surfaces are highly congruent.
With plantar flexion inverse movements occur: internal rotation of the fibula and talus,
tightening of the ATaFL,
relaxing of the PTaFL/CFL and anterior translation of the talus.
In this position the main stabilizer is the ATaFL.
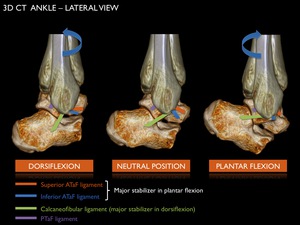
Fig. 12: Positioning of the lateral lower ligaments (ATaFL, CFL and PTaFL) in dorsiflexion, neutral position and plantar flexion of the ankle.
III.
RADIOGRAPHY IN ANKLE FRACTURES
In trauma setting a minimum of three plain films must be obtained : AP,
Mortise and lateral views.
An additional oblique view with the ankle in 45° internal rotation may be helpful.
At the AP radiograph we look at the distal tibiofibular overlap,
measured between the medial border of the fibular syndesmotic portion and the posterior malleolus of the tibia.
It should be greater than 6mm.
The medial clear space should be less than 3mm.
This should be equal to the horizontal clear space.
A widened medial clear space is suggestive for a tear in the deltoid ligament.
The Mortise view is done by internally rotating the tibia 15-20°.
In this view we can better appreciate the lateral clear space and syndesmotic space.
Here,
the lateral clear space must be less than 3-6 mm.
The distal tibiofibular overlap should be greater than 1mm.
The medial clear space has to be less than 4mm.
In a Mortise view of a normal ankle you may appreciate the fibular digital fossa.
This is not a normal finding on an AP view,
and suggests a tear (of variable degree) in the syndesmotic ligaments causing external rotation of the distal fibula.
The lateral view should show the distal fibula projecting over the posterior third of the distal tibia.
This is because the distal fibula is positioned more dorsally compared to the distal tibia.
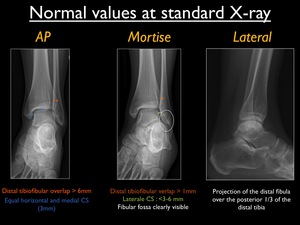
Fig. 13: Normal values at standard X-ray views (AP,Mortise and lateral)of the ankle.
IV.
PATHOGENESIS OF ANKLE INJURIES
Radiography not only shows fractures,
but may also give important information on ligamentous injury.
IV.A.
Concept of the greater ring
The talus is surrounded by bone and ligaments,
producing a ring (in the coronal plane) rendering stability.
The talus is the main key to ankle injuries.
All forces to the ankle are transmitted to the talus and from there transmitted to neighboring bones or ligaments.

Fig. 14: Coronal CT image of the ankle, illustrating the concept of the greater ring. The talus represents the center of the ring as key bone.
A single break (bone or ligament) in the greater ring does not produce ankle instability.
Two or more breaks (bone-bone,
bone-ligament,
ligament-ligament) in the greater ring generally lead to ankle instability.
Radiography may appear normal in an unstable ankle trauma,
with two ligamentous ruptures.
IV.
B.
Tissue failure patterns
Bones may fail through compression,
avulsion or torsion,
while ligaments may fail through rupture or avulsion (and rarely through compression).
A transsyndesmotic fracture line at the lateral malleolus with an oblique aspect (anteroinferior to posterosuperior) is caused by compression of the externally rotating talus and is called a push-off fracture.
At the medial malleolar side a push-off fracture is usually vertically oriented,
due to compression of the adducting talus.
A transverse fracture line in both lateral and medial malleoli,
is caused by avulsion or pulling of the talus through the ligaments.
This is called a pull-off fracture.
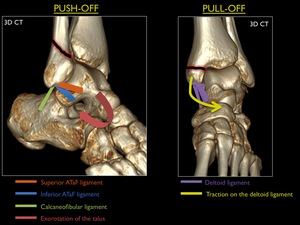
Fig. 15: 3D CT with illustration of the push-off and pull-off principle.
At the medial malleolus,
avulsion or pull-off fractures are more frequent than ruptures of the strong deltoid ligament.
At the lateral malleolus the opposite is true: compression or push-off fractures are more frequent than ruptures of the lateral ligaments.
Probably due to the fact that the individual lateral ligaments are not as strong as the bone.
IV.C.
Concept of the lesser ring
The syndesmotic ligaments form a lesser ring (in axial plane) together with the tibia and fibula,
which renders them stable.
A further connection exists in the central and posterior part,
respectively the interosseous and transverse inferior tibiofibular ligament.
Table 2 shows increasing degrees of instability due to one or more breaks in the lesser ring.
When the ATiFL,
IOL and PTiFL are torn,
the fibula rotates externally showing the pathologic digital fossa sign on the AP view.
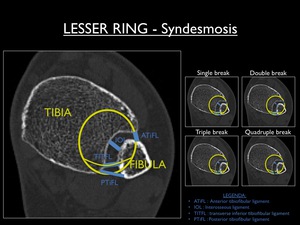
Fig. 16: Axial CT image of the ankle at the level of the syndesmotic ligaments, illustrating the concept of the lesser ring as well as the possible breaks.
| Type of break |
Instability |
| Single break (ATiFL)* |
Limited tibiofibular diastasis |
| Double break (ATiFL,
IOL) |
Moderate tibiofibular diastasis |
| Triple break (ATiFL,
IOL,
PTiFL) |
Severe diastasis |
| Quadruple (ATiFL,
IOL,
PTiFL,
TITFL) |
Total tibiofiular instability |
Table 2 : Classification of breaks in the lesser ring (* associated with at least partial tear of the IOL)
V.
CLASSIFICATION OF ANKLE FRACTURES
The most commonly used and well-known classification system is that of Weber.
It is a fairly easy system,
classifying fractures by its position in relation to the syndesmosis.
Three classes are being described: Weber A (or infra-syndesmotic),
Weber B (or transsyndesmotic) and Weber C (or suprasyndesmotic).
A second more detailed classification is the Lauge-Hansen classification,
in which the fracture is classified by explaining the trauma mechanism.
It describes how the foot and ankle move in different ankle injuries.
The classification is described in two parts.
The first part of the description is related to the position of the foot with respect to the body: supination (inversion) and pronation (eversion).
Supination stresses the lateral structures of the ankle,
while pronation stresses the deltoid ligament.
The second part of the description is related to the talar displacement or rotation: external rotation,
internal rotation,
abduction,
adduction and dorsiflexion.
There exists 5 major trauma mechanisms according to the Lauge - Hansen classification system,
explaing the vast majority of injuries: supination-external rotation,
supination-adduction,
pronation-external rotation,
pronation-abduction and pronation-dorsiflexion.
V.1.
Supination - External Rotation (SER)
This is the most common injury pattern,
with the foot in supination and external rotation of the talus due to transmitted force from the moving body through the talus.
With supination of the foot,
the ATiFL is under stress and as the forces continue the rotating talus pushes the lateral malleolus to posterior.
Four progressive stages are described:
SER Stage 1: Rupture of the ATiFL or avulsion at one of its insertions
SER Stage 2 : Stage 1 + transsydesmotic fracture of the fibula (push-off or Weber B) with a variable degree of damage to the syndesmotic ligaments
SER Stage 3: Stage 2 + rupture of the PTiFL or avulsion fracture of the posterior malleolus
SER Stage 4: Stage 3 + rupture of the deltoid ligament or avulsion fracture of the medial malleolus
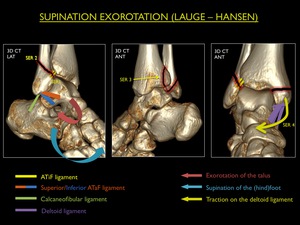
Fig. 17: Illustration of trauma mechanism "Supination - Exorotation" by Lauge - Hansen (stages 1-4).
Every higher stage indicates damage to the structures described in the lower stages.
If you see a transsyndesmotic fracture for example,
you should look at the ATiFL on MR.
It will be ruptured.
Major instability starts at SER stage 3,
and requires a transsyndesmotic screw if the syndesmosis is unstable at surgery.
V.2.
Supination - Adduction (SA)
This type of injury appears with the foot in supination and the ankle moving medially on the X-axis of the ankle (adduction).
Typically this injury is caused by missing a step.
It is the only mechanism explaining injury to the ATiFL (low lateral ligament) and consists of two stages:
SA Stage 1 : Rupture of the ATiFL or avulsion fracture of the fibula (transverse or Weber A)
SA Stage 2 : Stage 1 + compression fracture of the medial malleolus (vertical / push-off)
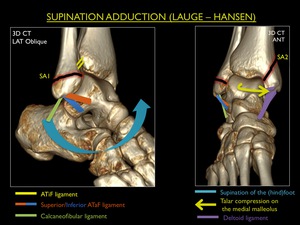
Fig. 18: Illustration of trauma mechanism "Supination - Adduction" by Lauge - Hansen (stages 1-2).
Stage 1 SA injuries are considered stable,
while a stage 2 SA is consistent with an instable fracture.
There also exists an inbetween stage (stage 1B), not described by Lauge-Hansen.
In this stage the ATiFL is ruptured and the adducting talus causes a bony bruise at the malleolus medialis (marrow edema at MR),
but is not strong enough to cause a real fracture.
This entity is mainly seen in children.
V.3.
Pronation - External Rotation (PER)
The PER is the most common eversion trauma of the ankle,
with the foot in pronation,
while the talus externally rotates due to transmitted force from the moving body through the talus.
The trauma begins at the medial side and with the rotation of the talus proceeds to the posterior and lateral ankle.
Because the medial side is the first being injured,
the talus can produce some degree of adduction in which it tears open the syndesmosis.
Four progressive stages are described:
PER Stage 1: Avulsion fracture of the medial malleolus or rupture of the deltoid ligament
PER Stage 2: Stage 1 + rupture of the ATiFL (or avulsion at its insertions) + any degree of injury to the lesser ring and distal interosseous membrane (explained higher up)
PER Stage 3: Stage 2 + suprasyndesmotic fracture of the fibula (transverse,
spiroid or comminuted)
PER Stage 4: Stage 3 + avulsion fracture of the posterior malleolus or rupture of the PTiFL
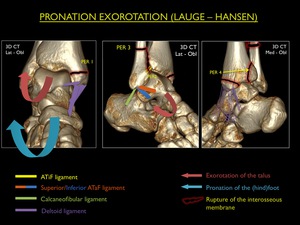
Fig. 19: Illustration of trauma mechanism "Pronation - Exorotation" by Lauge - Hansen (stages 1-4).
When the suprasyndesmotic fracture is located in the proximal fibula,
this is called a Maisonneuve fracture.
It means that the interosseous membrane is disrupted until the fibula breaks at the region of its lowest resistance.
Major instability starts at PER stage 3,
requiring a transsyndesmotic screw.
V.4.
Pronation - Abduction (PA)
This pattern of injury is uncommon.
It occurs with the foot in pronation and the talus moving laterally on the X-axis of the ankle (abduction) ,
leading to traction on the medial ankle structures and compression to the lateral malleolus.
The human body does not show a lot of velocity in this type of trauma (e.g.
coming down a stair),
explaining why the talus does not rotate.
Three stages of PA are described:
PA Stage 1: Avulsion fracture of the medial malleolus or rupture of the deltoid ligament
PA Stage 2: Stage 1 + rupture of the ATiFL and PTiFL (IOL intact) or avulsion at their insertions
PA Stage 3: Stage 2 + parasyndesmotic compression fracture
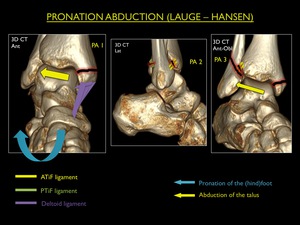
Fig. 20: Illustration of trauma mechanism "Pronation - Abduction" by Lauge - Hansen (stages 1-3).
It may be difficult to distinguish between PA stage I and PER stage I,
both showing identical pathology.
The compression fracture at the lateral malleolus in PA stage 3,
is typically oriented superolateral to inferomedial (due to push-off at the internal fibular side by the talus); while in SER it is oriented anteroinferior to posterosuperior (due to push-off at the anterior fibular side by the talus).
V.5.
Pronation-dorsiflexion (PD)
This type of mechanism related to the pilon or intra-articular (talocrural joint) comminuted fractures of the distal tibia.
Mainly osseous structures fail,
while ligaments are less affected.
Therefore CT is the best modality in evaluating these fractures.
In this injury,
the foot is in pronation and the ankle in dorsiflexion,
with axial loading.
The talus will be forced up into the tibiofibular fork,
causing fracture of the distal tibia.
These fractures typically occur during fall from a height,
motor vehicle accidents,
snow or waterski accidents.
Four progressive stages are described:
PD Stage 1: Fracture of the medial malleolus (usually vertical)
PD Stage 2: Stage 1 + fracture of the anterior margin of the distal tibia
PD Stage 3: Stage 2 + supramalleolar fracture of the fibula
PD Stage 4: Stage 3 + comminuted intra-articular fracture of the tibia
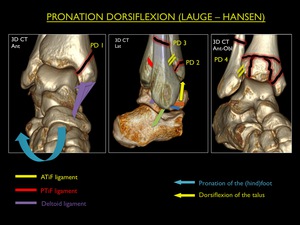
Fig. 21: Illustration of trauma mechanism "Pronation - Dorsiflexion" by Lauge - Hansen (stages 1-4).
After fracture of the medial malleolus,
the talus slightly luxates forward and its superior surface comes in contact with the anterior part of the distal tibial articular surface.
A large fragment from the anterior part of the distal tibia will be torn off,
if the trauma is powerful enough.
In summary,
the following flowcharts may guide you in the diagnosis of the correct mechanism and its stage.
In the absence of a fracture,
differentiation between PER with SA and PER with PA is impossible at radiography alone.
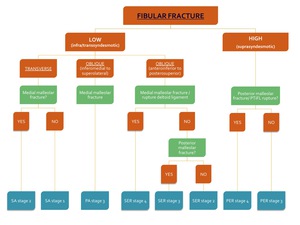
Fig. 22: Flowchart 1 showing the algorithm for the classification of an ankle fracture in the presence of a fibular fracture.
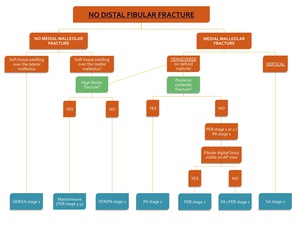
Fig. 23: Flowchart 2 showing the algorithm for the classification of an ankle fracture in the abscence of a distal fibular fracture.





 correlation of the superior and inferior ATaFL.")



.")


 in dorsiflexion, neutral position and plantar flexion of the ankle.")



.")
.")
.")
.")
.")

