In this section we will show several cases from our institution,
and where possible applying the Lauge-Hansen classification system in order to classify the injuries.
Using this system,
we can inform our clinician or orthopaedic surgeon on the possible lesions (bony and ligamentous) of the ankle.
CASE 1:
A 71 year old female patient presents at the emergency department with a "twisted" left ankle.
She missed a step walking on the street.
X-ray imaging was performed.
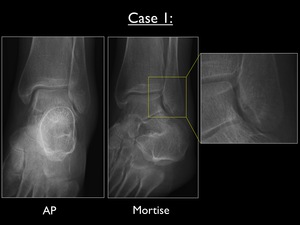
Fig. 24: AP and Mortise view of the left ankle in case 1, with enlarged focus on the discrete infrasyndesmotic transverse fracture line.
The AP and Mortise view of the left ankle show a discrete transverse fracture at the infrasyndesmotic lateral malleolus.
The fracture was not visible on the lateral X-ray image (not shown here).
This fracture is caused by avulsion or pull-off by the talus,
with the foot in supination and the talus in adduction (moves medially on the X-axis).
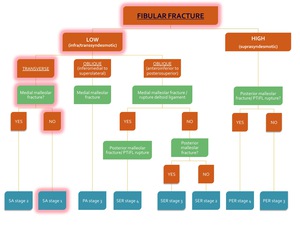
Fig. 25: Flowchart showing the algorithm for the classification of an ankle fracture in the presence of a fibular fracture. The path for diagnosis of SA stage 1 is highlighted in red.
Since there is no vertical fracture at the medial malleolus,
this is a stable fracture classified as Supination-Adduction stage 1 of 2 (see Fig. 18 below).
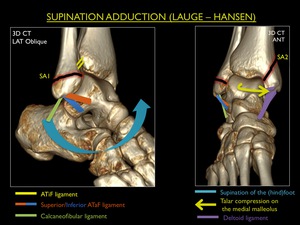
Fig. 18: Illustration of trauma mechanism "Supination - Adduction" by Lauge - Hansen (stages 1-2).
MR imaging can possibly show some degree of bone marrow edema at the medial malleolus/medial talar trochlea,
because of a bony bruise between both structures.
Ongoing talar adduction results in a vertical compression fracture of the medial malleolus : instable SA stage 2.
CASE 2:
A 38 year old male with an inversion trauma of the right ankle during soccer presents at the emergency department.
X-rays were performed.

Fig. 26: AP, Mortise and lateral view of the right ankle in case 2. Yellow arrows pointing out the obliquely oriented (anteroinferior to posterosuperior) transsyndesmotic fracture.
All images show a transsyndesmotic fracture at the distal fibula,
running from anteroinferior to posterosuperior,
as seen on the lateral view.
This fracture is caused with the foot in supination and a push-off by the externally rotating talus.
The medial and horizontal clear spaces are equal and less than 3 mm.
We may appreciate a fibular digital fossa on the AP view,
indicating a tear (of variable degree) in the syndesmotic ligaments causing external rotation of the distal fibula.
There is no posterior or medial malleolar fracture.
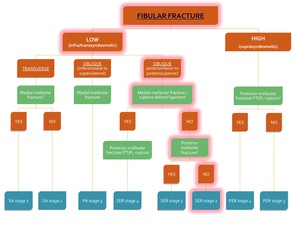
Fig. 27: Flowchart showing the algorithm for the classification of an ankle fracture in the presence of a fibular fracture. The path for diagnosis of SER stage 2 is highlighted in red.
This fracture is classified as Supination-Exorotation stage 2 of 4 and is stable (see flowchart).
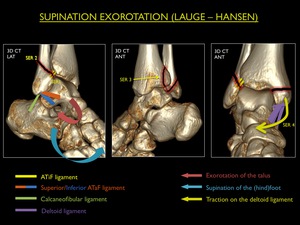
Fig. 17: Illustration of trauma mechanism "Supination - Exorotation" by Lauge - Hansen (stages 1-4).
Note : If an obliquely oriented fracture (anteroinferior to posterosuperior) is seen,
this could only have happened after rupture of the ATiFL.
When examining this kind of fracture on MR,
always look back at the ATiFL: it will be ruptured.
CASE 3:
A 27 year old male twisted his left ankle during athletics (sprint).
Clinical examination showed a deformation of the ankle for which X-ray imaging was performed.

Fig. 28: AP and lateral view of the left ankle in case 3. Yellow arrow = pull-off fracture of the medial malleolus - Blue arrow = suprasyndesmotic fracture - Purple arrow = cortical irregularity at the lateral side of the posterior malleolus
The AP view shows a transverse fracture at the medial malleolus and a comminuted suprasyndesmotic fibular fracture (Weber-C).
There seems to be a cortical irregularity at the lateral side of the posterior malleolus.
This can not be picked up on the lateral view.
There is no distal tibiofibular overlap (widening of the syndesmosis),
indicating major injury of the syndesmotic complex.
We suggested a CT since this is an obvious instable fracture and will require surgery.
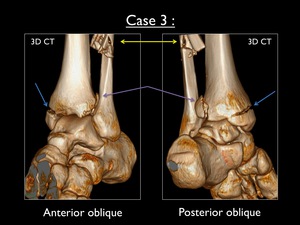
Fig. 29: Antero-oblique and postero-oblique 3D-CT images of the left ankle in case 3. Blue arrow = avulsion fracture of the medial malleolus - Yellow arrow = comminuted suprasyndesmotic fracture - Purple arrow = avulsion fracture at the lateral side of the posterior malleolus
3D CT imaging shows the medial and lateral fractures as seen on the X-rays.
This imaging modality has great benefit,
since it clearly shows the fracture at the posterior malleolus (doubtful on X-ray),
which possibly needs to be fixed by a screw.
This trauma is the result of a high velocity injury with the foot in pronation while the talus externally rotates.
The latter due to transmitted force from the moving body through the talus.
The trauma begins at the medial side and with the rotation of the talus proceeds to the posterior and lateral ankle.
Because the medial side is the first being injured,
the talus can produce some degree of adduction in which it tears open the syndesmosis.
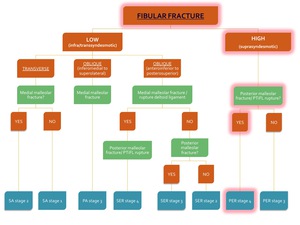
Fig. 30: Flowchart showing the algorithm for the classification of an ankle fracture in the presence of a fibular fracture. The path for diagnosis of PER stage 4 is highlighted in red.
This fracture is classified as Pronation-Exorotation stage 4 of 4 and is highly unstable (see flowchart).
A transsyndesmotic screw is mandatory.
Four progressive stages are described in this case:
PER Stage 1: Avulsion fracture of the medial malleolus
PER Stage 2: Stage 1 + rupture of the ATiFL + any degree of injury to the lesser ring and distal interosseous membrane (evaluated on MR)
PER Stage 3: Stage 2 + comminuted suprasyndesmotic fracture of the fibula
PER Stage 4: Stage 3 + avulsion fracture of the posterior malleolus
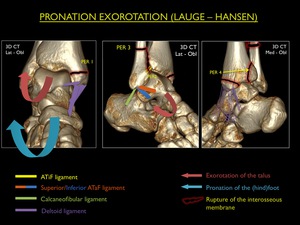
Fig. 19: Illustration of trauma mechanism "Pronation - Exorotation" by Lauge - Hansen (stages 1-4).
Note : In the presence of a Weber-C fracture,
always look at the previous checkpoints (medial malleolus/deltoid ligament and ATiFL): injury will be found at these sites.

Fig. 31: Postoperative AP and lateral view of the left ankle in case 3. Yellow arrow showing the fixation of the medial malleolus using 2 screws. Blue arrow showing the fixation of the fibular fracture using lateral plate and screws. No screw has been used in the posterior malleolus (purple arrow), due to too small fragment for fixation according to the orthopaedic surgeon.
CASE 4 :
A 78 year old female presents at the emergency department after a fall down the stairs.
Her ankle is deformed and X-rays were taken short after arrival.
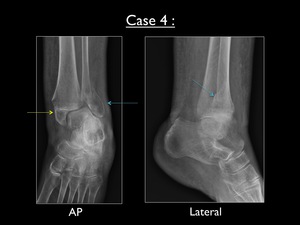
Fig. 32: AP and lateral view of the left ankle in case 4. Yellow arrow = avulsion fracture of the medial malleolus - Blue arrow = parasyndesmotic fracture (oriented from superolateral to inferomedial)
The plain films show a demineralized bone,
indicative of osteoporosis.
There is an avulsion fracture of the medial malleolus and a obliquely oriented parasyndesmotic fracture at the lateral malleolus.
The latter fracture line runs from superolateral to inferomedial.
This is an important finding in the differential diagnosis.
There is no fracture of the posterior malleolus.
The ankle stands in a pronated position.
The clue to the diagnosis is the orientation of the parasyndesmotic fracture line.
This type of fracture occurs with the foot in pronation and the talus moving laterally on the X-axis of the ankle (abduction),
leading to traction on the medial ankle structures and compression to the lateral malleolus.
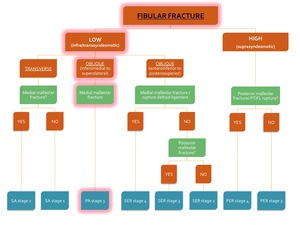
Fig. 33: Flowchart showing the algorithm for the classification of an ankle fracture in the presence of a fibular fracture. The path for diagnosis of PA stage 3 is highlighted in red.
This fracture is classified as Pronation-Abduction stage 3 of 3 and is unstable (see flowchart).
Following stages of PA are described in this case :
PA Stage 1: Avulsion fracture of the medial malleolus
PA Stage 2: Stage 1 + rupture of the ATiFL and PTiFL (IOL intact)
PA Stage 3: Stage 2 + parasyndesmotic compression fracture
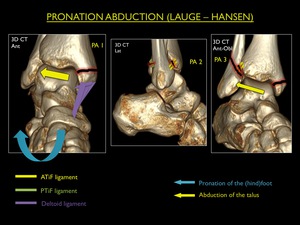
Fig. 20: Illustration of trauma mechanism "Pronation - Abduction" by Lauge - Hansen (stages 1-3).
Since this was an unstable fracture,
it has been treated surgically using osteosynthesis at the medial and lateral side.
The IOL is still intact,
so a transsyndesmotic screw was not necessary.
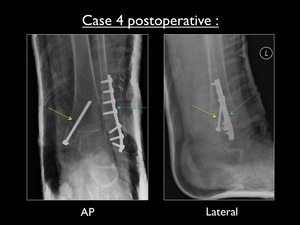
Fig. 34: Postoperative AP and lateral view of the left ankle in case 4. Yellow arrow showing the fixation of the pull-off fracture of the medial malleolus using one screw. Blue arrow showing the fixation of the fibular fracture using lateral plate and screws.
No transsyndesmotic screw was placed.
CASE 5:
This case shows a 60 year old female who ran away after being assaulted and fell down on the street.
Plain films were taken at our radiology department.
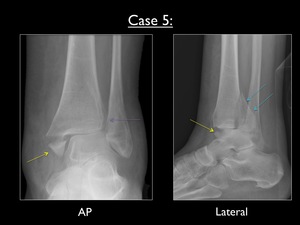
Fig. 35: AP and lateral view of the left ankle in case 5. Yellow arrow = avulsion fracture of the medial malleolus - Purple arrow = widening of the syndesmosis (normally distal tibiofibular overlap of > 6mm in AP and > 1mm in Mortise view) - Blue arrows = large avulsion fracture of the posterior malleolus
The AP view shows a transverse fracture at the medial malleolus (with obvious swelling of the soft tissue) and a widening of the syndesmotic joint.
Normally there should be overlap at the distal tibiofibular joint of > 6mm in AP and > 1mm in Mortise view.
The lateral image shows a large avulsion fracture of the posterior malleolus.
We suggested a radiograph of the upper fibula,
since there can't be a medial and posterior malleolar fracture without a fibular fracture.
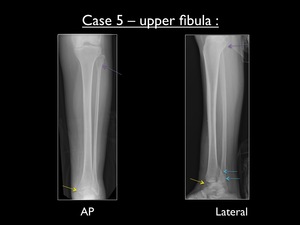
Fig. 36: AP and lateral radiograph of the left upper fibula, showing a high fibular fracture (purple arrow) in case 5. Yellow arrow = avulsion fracture of the medial malleolus - Blue arrows = large avulsion fracture of the posterior malleolus
The fracture pattern in this trauma is the result of a high velocity injury with the foot in pronation,
while the talus externally rotates.
The injury starts at the medial malleolus with a pull-off fracture or deltoid ligament tear.
This causes the lateral talar trochlea to move into the syndesmosis and with ongoing force tearing it open.
The interosseous membrane will be disrupted until the fibula breaks at the region of its lowest resistance.
When the suprasyndesmotic fracture is located in the proximal fibula,
this is called a Maisonneuve fracture.
In this case the talus keeps rotating externally,
causing an avulsion fracture of the posterior malleolus.
A CT was suggested to better appreciate the fractures pre-operatively.
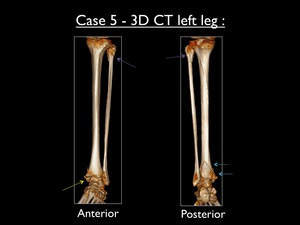
Fig. 38: Anterior and posterior 3D-CT views of the left upper fibula, confirming the high fibular fracture (purple arrow) in case 5. Yellow arrow = avulsion fracture of the medial malleolus - Blue arrows = large avulsion fracture of the posterior malleolus
It is a special case of Pronation - Exorotation stage 4 of 4and is considered unstable (see flowchart).
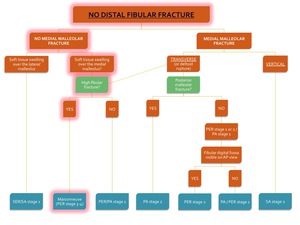
Fig. 37: Flowchart showing the algorithm for the classification of an ankle fracture in the absence of a distal fibular fracture. The path for diagnosis of a Maisonneuve fracture (in this case PER stage 4 with a posterior malleolar fracture) is highlighted in red.
Four progressive stages are described in this case:
PER Stage 1: Avulsion fracture of the medial malleolus
PER Stage 2: Stage 1 + rupture of the ATiFL + any degree of injury to the lesser ring and interosseous membrane
PER Stage 3: Stage 2 + comminuted fracture of the upper fibula
PER Stage 4: Stage 3 + avulsion fracture of the posterior malleolus
Fig. 19: Illustration of trauma mechanism "Pronation - Exorotation" by Lauge - Hansen (stages 1-4).
Note : Major instability starts at PER stage 3,
requiring a transsyndesmotic screw (used in this patient as well).
CASE 6:
A 40 year old male presented at the emergency department with a badly twisted ankle.
He heared several "cracks",
the ankle was considerably swollen and he was no longer able to stand on it.
X-ray imaging was performed.
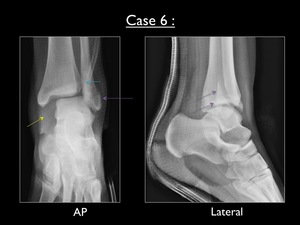
Fig. 39: AP and lateral radiograph of the left ankle in cast (case 6). Yellow arrow = significant increase of the medial clear space (>3mm) - Blue arrow = decreased tibiofibular overlap (<6mm) - Purple arrow = obliquely oriented (from anteroinferior to posterosuperior) transsyndesmotic fracture of the lateral malleolus
The AP view shows an obvious increase of the medial clear space (>3mm),
as well a decreased tibiofibular overlap.
The lateral view demonstrates an obliquely oriented transsyndesmotic fracture of the lateral malleolus,
running from anteroinferior to posterosuperior.
This latter finding is considered the signature of a supination - exorotation pattern.
There is no posterior malleolar fracture.
We suggested a CT in order to better evaluate the fractures.
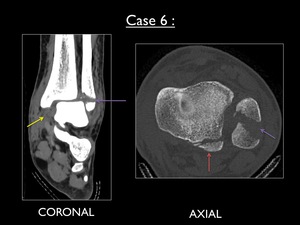
Fig. 40: Coronal (soft tissue) and axial (bone) CT images of the left ankle. Yellow arrow = rupture of the deltoid ligament with associated hematoma - Purple arrow = Weber-B type fracture - Red arrow = small avulsion fracture of the posterior malleolus (not seen on plain film)
The coronal image at CT shows a rupture of the deltoid ligament with a marked hematoma and secondary widening of the medial talofibular space.
The axial image at the level of the syndesmotic ligaments show the oblique distal fibular fracture,
as well as an avulsion fracture of the posterior malleolus.
The latter was not seen on plain film.
This fracture is classified as Supination - Exorotation stage 4 of 4 and is highly unstable (see flowchart).
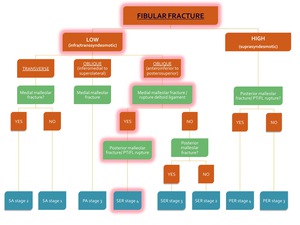
Fig. 41: Flowchart showing the algorithm for the classification of an ankle fracture in the presence of a fibular fracture. The path for diagnosis of SER stage 4 is highlighted in red.
This pattern occurs with the foot in supination and external rotation of the talus,
due to transmitted force from the moving body through the talus.
With supination of the foot,
the ATiFL is under stress and as the forces continue the rotating talus pushes the lateral malleolus to posterior.
Four progressive stages are described in this case:
SER Stage 1: Rupture of the ATiFL
SER Stage 2 : Stage 1 + transsydesmotic fracture of the fibula (push-off or Weber B) with a variable degree of damage to the syndesmotic ligaments
SER Stage 3: Stage 2 + avulsion fracture of the posterior malleolus
SER Stage 4: Stage 3 + rupture of the deltoid ligament
Fig. 17: Illustration of trauma mechanism "Supination - Exorotation" by Lauge - Hansen (stages 1-4).
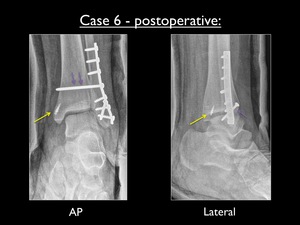
Fig. 44: Postoperative AP and lateral view of the left ankle in cast (case 6). Yellow arrow showing the fixation of the deltoid ligament using an anchor at the tibial side. Purple arrow showing the transsyndesmotic screw.
Note : Since we defined the pattern as SER and there was a rupture of the deltoid ligament,
there had to be injury to the posterior malleolus (bony avulsion or rupture of the PTiFL) as seen on the CT images.
CASE 7:
A 20 year old male patient enters the emergency department,
with a painful left ankle.
He went snowboarding the week before and landed quite hard on his left ankle after taking a high jump.
Standard plain fims were taken.
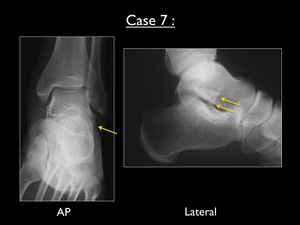
Fig. 42: AP and lateral radiograph of the left ankle (case 7). Yellow arrows = small bony fragment at the lateral process of the talus
On both AP and lateral view we can appreciate the presence of a small bony fragment at the lateral process of the talus.
We advised further imaging by CT.
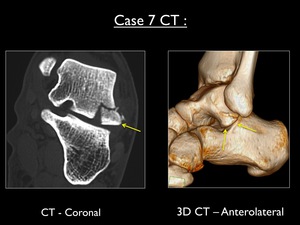
Fig. 43: Coronal CT (bone window) and anterolateral 3D-CT showing a bony fragment of 12mm originating from the lateral process of the talus (yellow arrow). Lateral displacement of 3mm was measured.
CT images (including 3D CT) confirm the presence of a bony fragment originating from the lateral process of the talus.
The inferior part of this structure is in contact with the posterior facet of the calcaneus,
while the superior part makes contact with the lateral malleolus.
It provides lateral stability to the ankle.
In supination and dorsiflexion of the (hind)foot combined with axial loading,
this talar segment becomes trapped in between calcaneus and lateral malleolus.
This is a typical presentation of a snowboarder's fracture.
Hawkins describes three subtypes:
Type 1 : avulsion (needs immobilization)
Type 2 : large fragment >1cm (needs ORIF)
Type 3 : Comminuted fragment (needs ORIF and excision of the small fragments)
Complications of non-treated snowboarder's fracture may include non-union,
malunion,
avascular necrosis and impingement.
Note: Important to remember as a radiologist is to describe displacement (>2mm is indicative for surgery) and the size of the fragment.
CASE 8:
A 14 year old girl presented at the emergency department after she twisted her left ankle during gymnastics.
X-ray imaging was performed.

Fig. 46: AP and lateral radiograph of the left ankle (case 8). Yellow arrows = vertical fracture at the distal tibial epiphysis - Purple arrow = possible displacement of the bony fragment.
The AP view of the left ankle shows a vertical fracture in the distal tibial epiphysis.
The fracture line starts at the growth plate and runs towards the tibiotalar joint.
We suspected an anterior displacement of the bony fragment on the lateral view.
Therefore we suggested further investigation of the fracture using CT imaging.
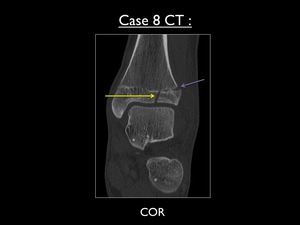
Fig. 45: Coronal CT (bone window) showing the vertical fracture at the anterolateral portion of the distal tibial epiphysis (yellow arrow) with lateral extension into the growth plate (purple arrow). No obviuos lateral or articular displacement is seen.
CT confirms the presence of a vertical fracture of the distal epiphysis into the growth plate and extending laterally,
which is called a juvenile Tillaux fracture.
There is no significant displacement.
This fracture is special since it is in fact an avulsion by the ATiFL at the tibial side.
It is the result of a supination - exorotation trauma mechanism (stage 1 of 4) in children.
The fusion of the distal tibial growth plate in children is irregular,
starting centrally at the tibial medial "hump" at an average age of 12,5 year over a period of 18 months.
From centrally it progresses medially,
posteriorly and finally the anterolateral part of the plate fuses ( Fig. 47 ).
The latter part is therefore prone to fracture,
while the fused parts become areas of relative strength.
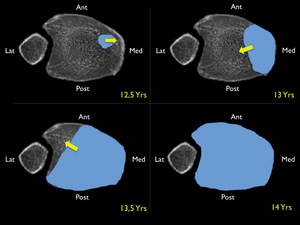
Fig. 47: Normal fusion pattern of the distal tibial growth plate ( blue dotted area) at increasing age (12,5yrs ; 13yrs ; 13,5yrs ; 14 yrs). Yellow arrow = direction of fusion.
Indications to osteosynthetic fixation are a lateral displacement of more than 2mm and/or an articular displacement.
These should be mentioned in the report of the radiologist.
Note: In adults a bony avulsion of the tibial insertion of the ATiFL can also occur,
and is called a Tillaux fracture.
An avulsion at the fibular insertion of the ATiFL is called a Wagstaffe-Lefort fracture.
These fractures occur due to the fact that the ligament is stronger than the bone.



.")
 transsyndesmotic fracture.")

.")



.")
, due to too small fragment for fixation according to the orthopaedic surgeon.")
")

.")

 - Blue arrows = large avulsion fracture of the posterior malleolus")
 in case 5. Yellow arrow = avulsion fracture of the medial malleolus - Blue arrows = large avulsion fracture of the posterior malleolus")
 is highlighted in red.")
 in case 5. Yellow arrow = avulsion fracture of the medial malleolus - Blue arrows = large avulsion fracture of the posterior malleolus")
. Yellow arrow = significant increase of the medial clear space (>3mm) - Blue arrow = decreased tibiofibular overlap (<6mm) - Purple arrow = obliquely oriented (from anteroinferior to posterosuperior) transsyndesmotic fracture of the lateral malleolus")
 and axial (bone) CT images of the left ankle. Yellow arrow = rupture of the deltoid ligament with associated hematoma - Purple arrow = Weber-B type fracture - Red arrow = small avulsion fracture of the posterior malleolus (not seen on plain film)")

. Yellow arrows = small bony fragment at the lateral process of the talus")
 and anterolateral 3D-CT showing a bony fragment of 12mm originating from the lateral process of the talus (yellow arrow). Lateral displacement of 3mm was measured.")
. Yellow arrow showing the fixation of the deltoid ligament using an anchor at the tibial side. Purple arrow showing the transsyndesmotic screw.")
 at increasing age (12,5yrs ; 13yrs ; 13,5yrs ; 14 yrs). Yellow arrow = direction of fusion.")