Fig. 9
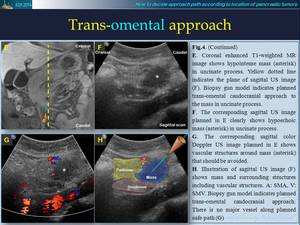
Fig. 10
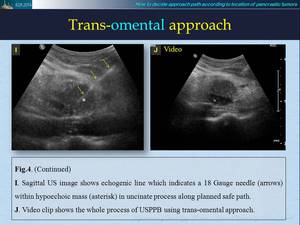
Fig. 11
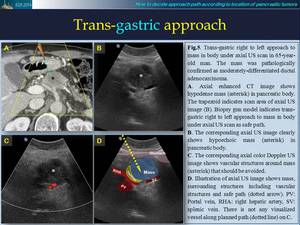
Fig. 12
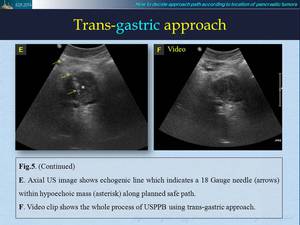
Fig. 13
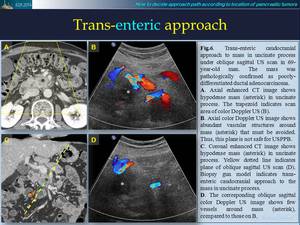
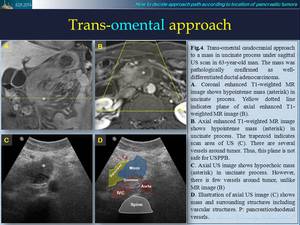
Fig. 14
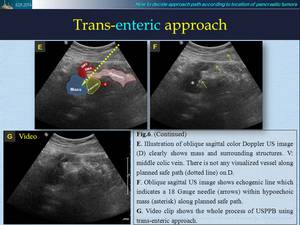
Fig. 15
Fig. 16
Fig. 17
Fig. 18
Fig. 19
Fig. 20
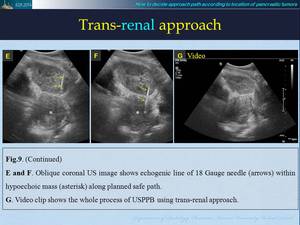
Fig. 21
Technical tips and tricks for safe and effective USPPB
How to select biopsy needle
Selection of adequate biopsy needle is very important for successful USPPB.
It affects successful acquisition of adequate target tissue.
A variety of needles with broad spectrums of calibers,
lengths,
and tip design are commercially available for percutaneous biopsy.
Needle caliber is important factor for successful USPPB.
In general,
small caliber needles (20 to 25 gauge) are used primarily to obtain specimens for cytologic analysis and large caliber needles (14 to 19 gauge) can be used to obtain greater amount of material for more thorough histologic analysis (7).
Recently,
among large caliber needles,
commercially available automated,
spring-loaded biopsy gun with 18 gauge needle has been preferable for abdominal biopsy.
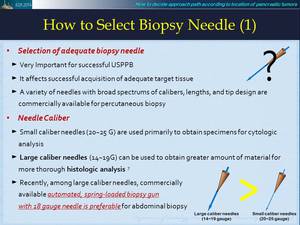
Fig. 22
Selection of biopsy needle with different sampling size depends on target size along biopsy path.
Biopsy gun with broad spectrum of sampling size is commercially available.
Biopsy gun with large sampling size is generally preferred when target is large and sufficiently thick for tissue cutting.
In contrast,
biopsy gun with small sampling size may be selected when target is small and thin.
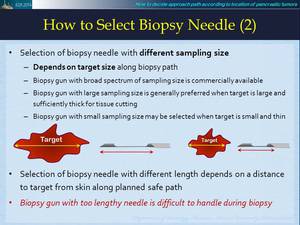
Fig. 23
Selection of biopsy needle with different length depends on distance to target from skin along planned safe path.
Biopsy needle with too long length is difficult to handle during biopsy.
Tips for Clear Visualization of Biopsy Needle
Key factors for safe and successful performance of USPPB are as follows; Clear visualization of biopsy needle during biopsy,
effectively handling of biopsy needle,
expertise of real-time US scanning,
experience of US guided percutaneous biopsy.
Fig. 24
Many operators prefer “free-hand” approach in which needle is freely inserted through skin under US imaging without imaginary guiding line.
Alignment of both needle tip and transducer should be parallel in free-hand technique.
For accurate free-hand technique,
it is very important that parallel placement of both needle and central ultrasound beam of transducer within same plane.
It allows entire needle shaft to be clearly visualized.
If needle was not visualized,
needle might be mis-aligned.
In this situation,
re-alignment by fine movement of needle along perpendicular direction of transducer under fixed transducer position can be a useful tip for clear visualization of biopsy needle.
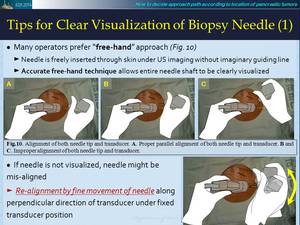
Fig. 25
Reflectivity of biopsy needle can affects USPPB performance.
Large caliber needles are more readily visualized than small caliber needles.
Thus,
this is one of reasons why large caliber needle such as 18 gauge needle is more preferred for USPPB.
Sometimes,
needle is not visualized on US images during biopsy,
even with large caliber needle used.
In this situation,
bobbing or in-and-out jiggling movement of biopsy needle during insertion of biopsy needle could improve needle visualization.
Bobbing motion makes trajectory of needle more discernible within otherwise stationary field.
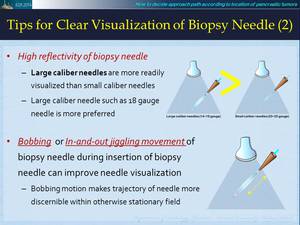
Fig. 26
The echotexture of structure which is being penetrated during biopsy also can affect visualization of biopsy needle.
Biopsy needles are easily identified within relatively hypoechoic structures such as liver,
spleen,
target masses and subcutaneous fat layer.
Presence of overlapping bowel gas or hyperechoic abdominal fat can render needle visualization difficult (Fig.11).
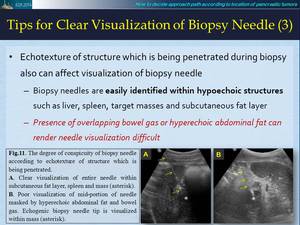
Fig. 27
How to effectively handle a biopsy needle
Expected penetration length of biopsy needle should be carefully considered during tissue cutting.
When using biopsy needle with double firing system,
first,
you can place needle tip at near edge of target lesion and then shoot single firing (advance inner cannula).
Second,
you can advance echogenic tip of inner cannula to desired depth within target for second firing of outer cutting cannula in a bid to cut target tissue.
It is very useful to avoid unexpected injury of deep seated critical structure such as vessel by over-penetration of target lesion during biopsy
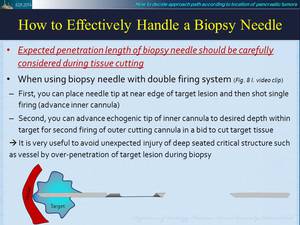
Fig. 28
