ECR 2014 / C-2377
Variant Angina: Assessment with Cardiac MDCT
This poster was previously presented at the 69th Korean Congress of Radiology (KCR 2013) in Seoul.
This poster is published under an open license. Please read the disclaimer for further details.
Congress:
ECR 2014
Poster Number:
C-2377
Type:
Scientific Exhibit
Keywords:
CT-Angiography, Vascular, Cardiovascular system, Cardiac, eLearning, Acute
Authors:
E. Lee1, S. I. Choi2, E. J. Chun2, Y. K. Kim3; 1Seongnam-si, Gyeonggi-do/KR, 2Seongnam-Si/KR, 3Seoul/KR
DOI:
10.1594/ecr2014/C-2377

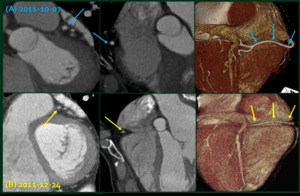
Fig. 1

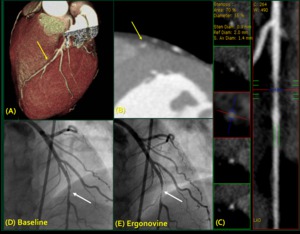
Fig. 2

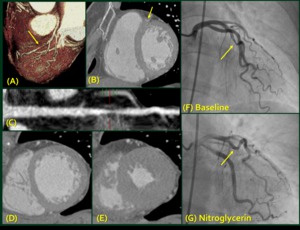
Fig. 3

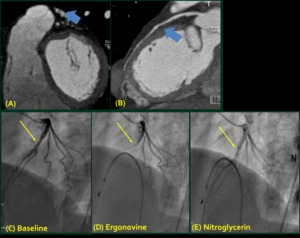
Fig. 4

Fig. 5