This poster is published under an
open license. Please read the
disclaimer for further details.
Keywords:
CT, Trauma, Emergency, Abdomen, Contrast agent-intravenous, Radiation safety
Authors:
R. Lakshmanan1, R. M. Mendelson2, S. Rao2, P. D. Fatovich2; 1Perth, Western Australia/AU, 2Perth/AU
DOI:
10.1594/ecr2015/C-0087
Methods and materials
Ethics approval
This was obtained from the Royal Perth Hospital ethics committee.
Inclusion criteria
- Patients presenting to Royal Perth Hospital emergency department with a history of,
or clinical corncern for abdominal trauma which warranted an abdominal CT.
- No contraindication to intravenous contrast.
- Completed study proforma.
- Consent form signed by patient or waiver of consent signed by next of kin.
Patient recruitment
Prospective recruitment of 41 cases who underwent the triple fractionated contrast injection protocol between December 2012 and October 2013.
Prospective recruitment of 41 controls who underwent the standard Royal Perth Hospital scanning protocol between December 2012 and September 2013.
Contrast injection method
- Pyelographic phase: >10 minutes prior to scanning,
40mL of Omnipaque 240 was hand injected in the emergency department by either the trauma registrar,
emergency registrar or radiology registrar.
- Patient was taken to CT.
- Portal venous phase: 85 seconds prior to scanning,
50mL of Omnipaque 350 or Optiray 350 was power injected at 4mL/ second.
- Arterial phase: 43 seconds prior to scanning,
70mL of Omnipaque 350 or Optiray 350 was power injected at 4mL/ second.
- Saline flush: 25.5seconds prior to scanning,
50mL of 0.9% normal saline was power injected at 2mL/ second.
- Scan commenced
- Single CT with combined enhancement in the arterial,
portal venous and pyelographic phases obtained.
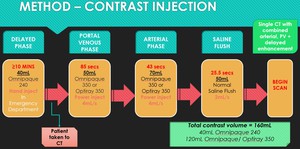
Fig. 2: Triple fractionated contrast injection protocol technique
References: Royal Perth Hospital, Radiology Department
See figure 2,
side bar for flow chart.
Fig. 2
Total contrast volume of 160mL used which included:
- 40mL of Omnipaque 240
- 120mL of Omnipaque/ Optiray 350
Protocol modifications for special circumstances
- CT head and/ or Cervical spine CT: The 40mL contrast bolus for the delayed phase was injected after the initial CT head and CT cervical spine were performed,
at least 10 minutes needed to elapse between giving the initial contrast bolus and commencement of scan.
- CT angiography of Head and Neck and / or Extremities: This was performed as a separate dedicated study after the body imaging had been completed.
Quality Scoring
- Quality scoring was performed on both patient populations.
- Anonymised cases were sent to three blinded case reviewers of different clinical experience,
including an abdominal and interventional radiology fellow; junior consultant abdominal radiologist (5 years subspecialty experience) and senior consultant abdominal and interventional radiologist (>20 years subspecialty experience).
- Each reviewer completed a quality scoring proforma for each patient.
Subjective quality scoring
- 5 subjective quality scoring measures were recorded for each patient who underwent the new triple fractionated contrast injection protocol.
This was performed using a 0 - 10cm visual analog scale,
see Fig. 3.
- Subjective scores of quality of the arterial phase enhancement,
portal venous phase enhancement,
systemic venous enhancement and pyelographic enhancement were recorded.
- An overall subjective quality score was also provided.
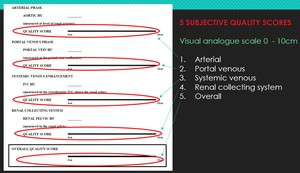
Fig. 3: Subjective quality scoring
References: Royal Perth Hospital, Radiology Department
Objective quality scoring
- 4 objective quality scoring measures were recorded for each patient in both population groups,
see Fig. 4.
- Objective hounsfield unit measurements were obtained at specific levels on each scan at the following sites; aorta at the level of the renal arteries; portal vein measured at the confluence; extrahepatic IVC above the renal veins; and the best enhancing renal pelvis.
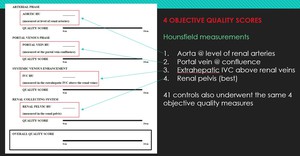
Fig. 4: Objective quality scoring
References: Royal Perth Hospital, Radiology Department
Radiation dose calculations
- Dose reports for each study were reviewed with mAs,
kVp,
DLP and CTDI recorded.
- Effective doses were calculated for the abdominal scan for each patient using the conversion factors described by Huda et.
al.3
Follow up
All patients who underwent the triple fractionated injection protocol were followed up through a review of the clinical notes and discharge summaries.



