I.
RADIOGRAPHIC EXAMINATION:
Role of conventional radiology:
- first modality of choice in the evaluation of the knee (a,
Langenskiöld staging; b,
angle measurements)
- differential diagnosis
- follow-up.
1.
a.) Langenskiöld stages are age dependent progressive stages,
based on the degree of depression of the medial plateau [1,
5,
6] (Fig.
2):
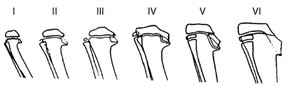
Fig. 2: Stages of Blount-disease. Age dependent, progressive changes of the medial tibial epiphyseal plate, meta- and epyphyisis.
References: Langenskiöld (1952) Acta Chir Scand 103:1
- Stage I.: BEAK,
2-3 years,
medial metaphyseal beaking
- Stage II.: SAUCER,
2-4 years,
saucer shaped defect of the medial metaphysis
- Stage III.: STEP,
4-6 years,
saucer deepens into step
- Stage IV.: BENT PLATE,
5-10 years,
epiphysis bent down over the medial beak
- Stage V.: DOUBLE EPIPHYSIS,
9-11 years
- Stage VI.: OSSIFIED MEDIAL EPIPHYSIS,
10-13 years,
development of medial physeal bony bar
1.
b.) Angle measurements [1,
5,
7]
- meta-diaphyseal (Drennan) angle (Fig.
3)
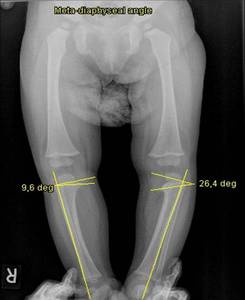
Fig. 3: Meta-diaphyseal angle measurement in infantile Blount-disease.
The metaphyseal-diaphyseal angle is defined as the angle between a line perpendicular to the axis of the tibia and a line through the most distal ossified beak of the medial and lateral tibial metaphysis.
Normal angle on the right side, abnormally wide angle and medial tibial metaphyseal beaking on the left side.
The normal value of meta-diaphyseal angle is less than 110.,
in Blount-disease it exceeds 110.
- tibiofemoral angle (Fig.
4)
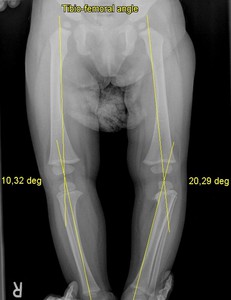
Fig. 4: Tibiofemoral angle measurement in infantile Blount-disease.
Normal angle on the right side and abnormal widening of the tibiofemoral angle on the left side.
In Blount-disease the tibiofemoral angle exceeds 150.
Normally it is less than 150.
The orthopedic treatment planning is typically established on plain radiographs by measuring the angles and assessing the medial aspect of the proximal tibial physis.
A child younger than 4 years of age,
with Langenkiöld stage I-II.
Blount-disease and a meta-diaphyseal angle greater than 110,
but less than 300 is usually treated with bracing,
called KAFO (knee-ankle-foot orthesis). Surgical correction of infantile Blount-disease is considered after the age of 4-5 years,
if the deformity has not corrected with bracing [8].
A meta-diaphyseal angle above 300,
combined with a tibiofemoral angle exceeding 150 means relative indication for orthopedic surgery.
2.
Differential diagnosis
The main differential of infantile Blount-disease is physiologic genu vara [9] Fig.
5).
In newborns there is a physiologic varus angulation in the knee joint,
which can measure up to 170.

Fig. 5: Radiograph of physiologic genu vara in an infant.
With normal growth and mechanical use of the lower extremities,
physiologic genu vara will turn into a 50 valgus after the age of three [10,
11] (Fig.
6).
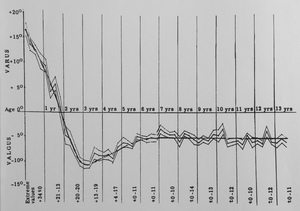
Fig. 6: Development of the tibiofemoral angle in children during growth.
References: Salenius P, Vanka E. Bone Joint Surg 1975;57(A):259-61.
Compared to physiologic bowing where the maximum angulation is exactly at the level of the knee joint,
in Blount-disease,
the angulation is located to the proximal aspect of the tibia.
3.
Follow-up examination
Further radiographic imaging is performed to evaluate progression and follow-up conservative or surgical treatment (Fig.
7,8,9).

Fig. 7: Infantile bilateral Blount-disease.
Radiographs of the same female patient at the age of 3 and 5 years.
Images show severe flattening of the medial tibial epiphysis on both sides. There are longitudinal low-attenuation areas in the beak-shaped medial tibial metaphysis, which might be due to the invanginations of cartilage into the metaphysis. Follow-up examination shows progression of tibia vara.

Fig. 8: Infantile unilateral Blount-disease.
Radiographs of the same girl with left sided tibial involvement at the age of 15 months and 6 years. Surgery was performed at 3 years of age.
The pre-operative radiographs show irregularity and widening of the tibial growth plate, with metaphyseal beaking and severe varus deformity on the left side keeping with infantile type of Blount-disease.
After proximal tibial osteotomy, the tibiofemoral and meta-diaphyseal angles are within the normal range, but there is an irreversible damage to ossification.

Fig. 9: Blount-disease, late onset form, unilateral involvement.
Plain radiographs of the right knee of a male patient show that the width of the tibial epiphysis is slightly diminished at its medial aspect, the growth plate is widened. The distal femur shows an irregular growth plate laterally. Considering the follow-up radiograph, there is no significant change.
II.
MAGNETIC RESONANCE IMAGING:
Role of MRI:
- Second choice of imaging method in Blount-disease,
mainly for operative treatment planning.
- Evaluation of physeal cartilage,
the pattern of physeal closure,
menisci,
ligaments.
MRI is mainly performed before surgical intervention,
for the evaluation of the physeal cartilage,
femoral involvement and additional meniscal and ligamentous changes [8,
12] (Fig.
10,
11,
12).
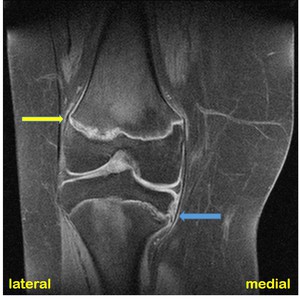
Fig. 10: Late onset type Blount-disease. Unilateral involvement. Same patient's radiographs shown in Fig. 9.
T1FS-weighted coronal MR image of the right knee of a 16 years old male patient.
There is mild flattening of the medial tibial epiphysis. The medial tibial metaphysis has a beak shape. The medial tibial growth plate is irregular and widened (blue arrow). Similar growth plate changes are visible at the lateral aspect of the distal femur (yellow arrow).
Note the wide subcutaneous fat (obesity as risk factor).
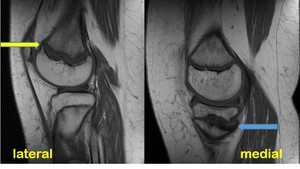
Fig. 11: Late onset type Blount-disease. Unilateral involvement. Same patient's radiographs shown in Fig. 9.
T1-weighted sagittal MR images of the right knee of a 16 years old male patient.
The medial tibial growth plate is irregular and widened (blue arrow). Similar growth plate changes are visible at the lateral aspect of the distal femur (yellow arrow).

Fig. 12: Late onset type Blount-disease. Unilateral involvement. Same patient's radiographs shown in Fig. 9.
T2STIR-weighted coronal MR images of the right knee of a 16 years old male patient.
There is high signal in the distal lateral femoral metaphysis, in keeping with bone marrow edema (yellow arrow), which might be due to the changed mechanical forces.
Evaluating 18 knee MRI-examinations of children with infantile Blount-disease,
Ho-Fung et al found that the most severe abnormalities occur in the medial compartment of the knee.
However the lateral compartment is often affected [12].
Coronal gradient echo and T1-weighted sequences proved to be the most useful for the visualization of the epipyseal cartilage.
MRI provides detailed information regarding the extent of growth-plate involement.
Documenting a physeal bar and the status of the medial joint (early degenerative changes,
meniscal tear) are important for surgical planning and prognosis.
The method of sugical intervention (tibial-,
fibular-,
femoral osteotomy,
internal- or external fixation,
+/- epiphyseodesis) is considered individually. If an epiphyseodesis is performed,
the contralateral knee should be evaluated to predict future leg-length discrepancies and epiphyseodesis of the contralateral knee should be considered [8].
