ISCHIOFEMORAL IMPINGEMENT
Ischiofemoral impingement is defined by hip pain related to narrowing of the space between the ischial tuberosity-hamstring tendon unit medially and lesser trochanter laterally,
with intermittent compression of the quadratus femoris muscle (QFM) and associated edema,
tears or fatty replacement.
[3,4] Fig. 1
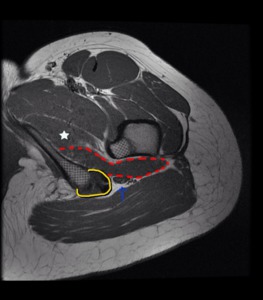
Fig. 1: Axial proton density-weighted MR image of left hip shows the anatomic relationship of QFM (dotted red line) in the ischiofemoral space. The QFM is a flat and quadrilateral shaped muscle located between the ischial tuberosity medially and femoral lesser trochanter laterally (crossed lines). It arises from the upper part of the lateral border of the ischial tuberosity, just anterior to the hamstring tendon origin (bordered by the yellow line), and inserts at the intertrochanteric crest on the posterior aspect of the proximal femur. Anteriorly, the QFM is bordered by the obturator externus muscle (star) and posteriorly it is bordered by fat and the sciatic nerve (blue arrow).
References: References: Radiology, Unidad Central de Radiodiagnóstico, Hospital Infanta Leonor - Madrid/ES
The ischiofemoral narrowing may be positional,
acquired or congenital.
Positional factors that may cause ischiofemoral narrowing include lower extremity internal/external rotation,
adduction/abduction,
and flexion/extension.
Congenital ischiofemoral narrowing causes may include a lower ischiopubic ramus,
prominent lesser trochanter,
larger cross section of the femur at the level of the lesser trochanter,
more posteromedial position of the femur,
or the common configuration of the female pelvic osseous anatomy (which shows greater width and lesser anteroposterior dimensions when compared to males).
Finally,
acquired ischiofemoral narrowing may be seen secondary to prior fractures of the lesser trochanter,
intertrochanteric valgus osteotomy,
expansile bone lesions (eg,
osteochondroma),
QFM atrophy,
enthesophytes extending laterally from the proximal hamstring origin or osteoarthritis changes leading to superomedial migration of the femur.
[1,4,6,7]
The ischiofemoral narrowing can be evaluated by measuring the following spaces:
-
Ischiofemoral space (IFS): The smallest distance between the lateral cortex of the ischial tuberosity and the medial cortex of the lesser trochanter.
-
Quadratus femoris space (QFS): The smallest space for passage of the QFM bordered by the superolateral surface of the hamstring tendons and the posteromedial surface of the iliopsoas tendon or lesser trochanter.
(performing the measurements on axial MRI images through the lesser trochanter).
[4,6,7] Fig. 2
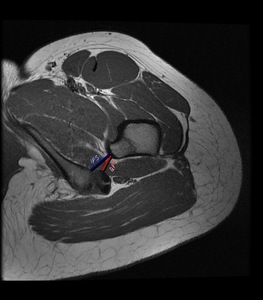
Fig. 2: Axial proton density-weighted MR image of left hip shows normal ischiofemoral space (IFS-blue line) and quadratus femoris space (QFS-red line).
References: References: Radiology, Unidad Central de Radiodiagnóstico, Hospital Infanta Leonor - Madrid/ES
With the hip in adduction,
external rotation and extension,
the normal distance between lesser trochanter and ischial tuberosity (IFS) proposal by some authors is about 2.0 cm.
The prevalence of a narrowed IFS and QFS in asymptomatic patients is unknown.
However,
two studies have shown that in patients with symptomatic ischiofemoral impingement,
the distances of IFS and QFS are significantly reduced compared with control individuals:
|
|
Symptomatic patients
|
Control patients
|
|
Hip in internal rotation [7]
|
IFS: 13±5 mm
QFS: 7±3 mm
|
IFS: 23±8 mm
QFS: 12±4mm
|
|
Hip in neutral position [6]
|
IFS: 12.9±3.7 mm
QFS: 6.71±2.7 mm
|
IFS: 29.3±5.9 mm
QFS: 13.5±4.5 mm
|
Some caution is advised in daily practice,
because the measurements depend on the degree of hip rotation,
adduction and extension during image acquisition.
MRI acquisition with hip in external rotation must be avoided as this may lead to overestimation of IFS and QFS narrowing.
[3,7]
- Clinical presentation
-
more common in women
-
patients affected are usually older than patients with other types of hip impingement,
with a mean age of 51–53 years (although it can affect all ages,
ranging from 11 to 77 year)
-
nonspecific chronic pain in the hip,
groin and/or buttock without a history of traumatic injury
-
distal radiation of pain to the posterior thigh and knee is not uncommon likely due to irritation of the adjacent sciatic nerve (sciatic radiculopathy symptoms) Fig. 4 Fig. 5
-
snapping sensation or locking in the joint
-
there is no specific clinical test on physical examination,
although pain may increase with wide range of hip positions: may be reproduced by a combination of hip extension,
adduction and external rotation or with flexion and internal rotation
[1,2,4,6,7]
- Diagnosis and imaging findings
The diagnosis of ischiofemoral impingement is largely dependent on imaging studies,
especially on MR images,
even though radiologic findings should be interpreted with caution.
It is very important correlate radiologic findings with clinical history and physical examination due to narrowing of IFS,
with or without QFM edema or atrophy,
may be an incidental finding in asymptomatic patients or severe clinical symptoms are not always related to narrower spaces.
In fact,
it is not uncommon that patients present with bilateral IFS narrowing with mild QFM edema and unilateral hip pain.
On the other hand,
symptomatic patients with QFM edema have been observed with normal space measures (although some of these patients may have a traumatic QFM tear rather than impingement).
[3,7,8]
Plain radiographs of the hip in these patients are usually normal,
although chronic osseous changes such as sclerosis and cystic changes of the lesser trochanter and the ischium may be present.
[1,4] Fig. 3

Fig. 3: A 45-year-old man with six month history of right groin. Right hip radiographs views show chronic osseous changes of ischiofemoral impingement, with sclerosis and subcortical cystic changes of the lesser trochanter and the ischium (blue arrow).
Axial proton density-weighted fat-suppressed MR image of the same patient shows edema within QFM(curved arrow)and subcortical cystic changes with edema in the ischial tuberosity (thin blue arrow).
References: References: Radiology, Unidad Central de Radiodiagnóstico, Hospital Infanta Leonor - Madrid/ES
A routine hip or pelvis protocol of MR imaging is the standard method to diagnose ischiofemoral impingement (best seen on axial images).
Changes suggestive of ischiofemoral impingement include a reduced IFS and/or QFS with deformity and edema (minor or moderate degree in most patients) or partial tears,
centered on QFM belly at the site of maximal impingement,
which may be unilateral or bilateral.
With increased severity of impingement,
edema becomes more severe and diffuse and may involve the surrounding soft tissues.
[3,4,7] Fig. 3 Fig. 4 Fig. 5 Fig. 6
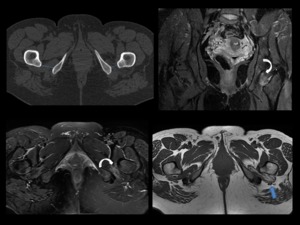
Fig. 4: A 42-years-old woman with a one year history of left hip pain and distal radiation of pain to the posterior knee.
Axial CT and MR images (coronal proton density-weighted fat-suppressed, axial T2-weighted fat suppressed and axial T1-weighted) demostrate ischiofemoral impingement in left hip with narrowed IFS(blue line in CT), diffuse edema with moderate fatty infiltration of QFM (curved arrow) and mass effect of QFM on sciatic nerve(blue arrow).
References: References: Radiology, Unidad Central de Radiodiagnóstico, Hospital Infanta Leonor - Madrid/ES
Additional imaging findings present in ischiofemoral impingement that we can find are:
-
edema surrounding the iliopsoas tendon insertion
-
edema and tears affecting the hamstring tendons Fig. 5
-
bone marrow edema,
sclerosis or cystic change of the ischium/lesser trochanter Fig. 3
-
bursa-like formation Fig. 6
-
or muscle atrophy with fatty infiltration (in patients with long-standing ischiofemoral impingement) Fig. 7
[1,3,4,6,7]
Differential diagnoses,
such as a strain or tear of the quadratus femoris muscle without ischiofemoral impingement must be ruled out by performing a precise clinical history.
One morphologic feature that might help in differentiating these entities at MRI is the fact that edema from a tear or strain most commonly occurs at the musculotendinous junction,
whereas the muscle edema in ischiofemoral impingement is diffuse or at the site of maximal impingement.
The clinical history of acute onset of pain associated with activity or the absence of IFS narrowing lead away from a diagnosis of ischiofemoral impingement.
[3,9]
-Treatment
Nowadays, no definitive treatment strategy for ischiofemoral impingement has been established.
The first option is a conservative treatment that includes activity restriction,
anti-inflammatory medications and rehabilitation exercises.
The second option is a ultrasound o CT-guided steroid and/or local anesthetic injection within the ischiofemoral space.
Finally,
in those patients in whom pain is refractory to conservative treatment,
surgical intervention may be considered,
with open decompression of the ischiofemoral space by excision of the lesser trochanter.
[1,6]
ANTERIOR INFERIOR ILIAC SPINE/SUBSPINE IMPINGEMENT
Anterior inferior iliac spine or subspine impingement is a recent emergent diagnosis caused when the anterior aspect of the femoral head and neck impacts the anterior inferior iliac spine (AIIS) as a result of AIIS hypertrophy,
prior avulsion injuries or pelvic osteotomies.
The AIIS apophysis arise just above the level of the anterosuperior acetabular rim and is the origin of the direct head of the rectus femoris.
[1,2,3,10] Fig. 8
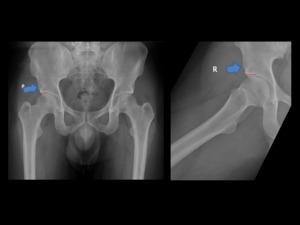
Fig. 8: An anteroposterior and frog-leg lateral radiographs showing the localization of AIIS (blue arrow), just above the anterosuperior acetabular rim (red line) with normal appearance.
References: References: Radiology, Unidad Central de Radiodiagnóstico, Hospital Infanta Leonor - Madrid/ES
It has a variable morphology.
Hetsroni et al.
described a method to classify the AIIS into three morphological types based on the relationship between the distal extension of the AIIS and the anterosuperior acetabular rim: type I,
in which there is a smooth ilium wall between the most caudad level of the AIIS and the anterosuperior acetabular rim,
without bone prominence Fig. 9; type II,
in which the AIIS prominence extended to the level of the acetabular rim Fig. 10; and type III,
in which a prominent AIIS extended distally to the acetabular rim Fig. 11.
Type II and Type III variants are associated with a decrease in hip flexion and internal rotation and could be involved in the subspine impingement.
[11]
Prominence of the AIIS with excessive distal and/or anterior extension can be:
-
developmental and seen in association with acetabular retroversion;
-
traumatic,
due to prior apophyseal or rectus femoris tendon avulsions,
-
or over-correction after periacetabular osteotomy.
Although most patients with an avulsion injury of the AIIS have a good response to conservative treatment,
in some patients the inferior displacement of the apophysis can lead to malunion which results in an enlarged AIIS.
Repeated contact between this abnormally hypertrophic AIIS and the distal femoral neck,
mainly with hip flexion movement,
is supposed to be the cause of this form of extra-articular hip impingement secondary to a mechanical conflict.
[1,3,12]
- Clinical presentation
-
patients are typically 14–30 years-old with strong male predominance
-
actively involved in sports
-
anterior hip or groin pain that occurs with straight hip flexion or with prolonged hip flexion
-
anterior hip pain aggravated by activities such as sprinting and kicking (eg.
soccer)
-
limitation in range of passive hip straight flexion on physical examination
-
tenderness over the AIIS
-
only partial pain relief after intra-articular anesthetic injections
[1,2,3,10]
- Diagnosis and imaging findings
Pelvic x-rays and CT scans with 3D reconstruction images play a capital role in the diagnosis of this atypical form of extra-articular hip impingement and are invaluable to the orthopedic surgeon in the preoperative assessment.
MR imaging may also demonstrate abnormalities of the AIIS or subspine region,
but its role is secondary in this condition Fig. 12.
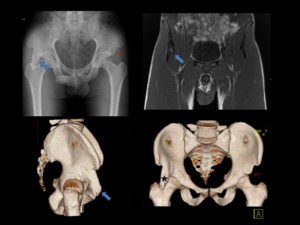
Fig. 12: A 28-years-old man with right groin pain during hip flexion and decreased range of motion after sport injury five years ago (soccer player).
Anteroposterior pelvis radiographs, 3D CT reconstruction and coronal T1-weighted MR images demonstrate prior avulsion injury of the AIIS with secondary deformity and bony hypertrophy (blue arrow), extending caudad to the level of the anteriorsuperior acetabular rim (type III variant). He was diagnosed with subspine impingement in the right hip.
Note that on left side, AIIS is slightly enlarged after prior similar injury (red arrow), but osseous protrusion is smaller (type II variant).
References: References: Radiology, Unidad Central de Radiodiagnóstico, Hospital Infanta Leonor - Madrid/ES
Pelvis or hip radiographs and CT images may demonstrate:
-
AIIS deformity with bony hypertrophy (as a result of prior displaced avulsion fracture) Fig. 12 Fig. 14
-
calcified deposits within the proximal portion of the straight head of the rectus femoris tendon (secondary to rectus femoris tendon pathology) Fig. 15
-
extension of AIIS to the level or below the level of the anteriorsuperior acetabular rim Fig. 12 Fig. 14
[1,3,12] Fig. 12
Occasionally cyst in the femoral neck can be found but more distal than those found in FAI.
[1,10,12]
A case series has shown that concomitant cam type of FAI was present in eight of ten patients with surgically proven subspine impingement [10] and asymptomatic heterotrophic ossification has been described.
[2]
Consequently,
it is essential to assess our radiologic findings within the clinical context of each patients in order to reach a final diagnosis and therefore a more accurate management.
-Treatment
Surgical management of subspine impingement consists of an arthroscopic decompression of a symptomatic prominent AIIS deformity that results in improved hip motion and hip function.
[10] Fig. 12 Fig. 13
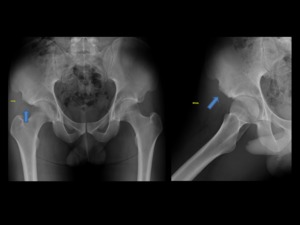
Fig. 13: Same patient as in Fig.12 Anteroposterior and frog-leg lateral radiographs views following arthroscopic decompression of the hypertrophic AIIS (blue arrow). Patients was able to return to training and competition at 6 months after the surgery.
References: References: Radiology, Unidad Central de Radiodiagnóstico, Hospital Infanta Leonor - Madrid/ES
ILIOPSOAS IMPINGEMENT
Iliopsoas impingement is a new arthroscopic diagnosis refers to an acetabular labral tears at the anterior location (3-o’clock position) thought to be caused by the iliopsoas tendon.
Fig. 16
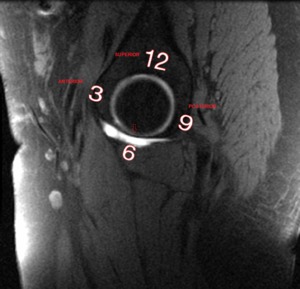
Fig. 16: Sagittal T1 fat saturated MR arthrographic image. Schematic drawing on the right hip used to localization of labral tears (clock-face localization). The transverse acetabular ligament (red arrow) is define as 6 o´clock (inferior).
References: References: Radiology, Unidad Central de Radiodiagnóstico, Hospital Infanta Leonor - Madrid/ES
In FAI and other pathological conditions such as trauma,
dysplasia,
degeneration and hypermobility,
labral tears occur mostly in the typical anterosuperior position (1- through 2 o’clock position).
[2,13,14] Fig. 16
In a recent arthroscopic study,
Domb and colleagues [13] reported a distinct pattern of labral abnormality,
with localized labral damage anteriorly that did not extend to the anterosuperior portion of the acetabulum and that was directly adjacent to the iliopsoas tendon.
Several theoretical explanations for this atypical 3-o’clock position labral injury have been proposed:
-
a tight or inflamed iliopsoas tendon causing impingement of the anterior labrum during hip extension,
-
an iliopsoas tendon that has become scarred or adherent to the anterior capsule-labral complex and leads to repetitive traction injury,
-
or a hyperactive iliocapsularis muscle causing a traction injury of the capsular-labral complex.
[3,13]
This entity is a novel diagnostic entity that differs from:
- internal coxa saltans,
a hip pathology secondary to extra-articular iliopsoas tendon snapping with a painful anterior hip clicking sensation that is reproducible on physical examination
- iliopsoas impingement after total hip arthroplasty,
a hip disorder involving the iliopsoas tendon due to friction against a misaligned or oversized prosthetic acetabular component.
- Clinical presentation
-
average age of patients with iliopsoas impingement is 25–35 years (range,
15–57 years) with strong female predominance
-
anterior hip or groin pain that gets worse with hip flexion and prolonged sitting
-
a positive impingement test (pain with passive flexion,
adduction,
and internal rotation)
-
nonspecific focal tenderness over the anterior hip area and iliopsoas tendon at the level of the anterior portion of the joint.
[13,14]
- Diagnosis and imaging findings
Iliopsoas impingement may not be clinically suspected because there are no specific clinical or imaging findings to reach this diagnosis,
so very often the diagnosis is made at the time of arthroscopic hip surgery.
Iliopsoas impingement at hip arthroscopy is diagnosed when there is inflammation,
deformation,
tearing,
or mucoid degeneration of the labrum at the 3-o’clock position,
located directly beneath the iliopsoas tendon,
with no evidence of any other known cause of labral injury (femoroacetabular impingement,
trauma,
dysplasia,
capsular laxity,
or osteoarthritis).
There can also be associated focal synovitis.
[1,13,14]
Although specific imaging criteria are still being refined,
a recent study by Blankenbaker and colleagues [14] concludes that,
without radiologic evidence of dysplasia or FAI,
an isolated anterior acetabular labral tear found at MR arthrography at the 3 o’clock position should suggest the diagnosis of iliopsoas impingement,
especially if the tear does not extend above the 2 o’clock position.
Other parameters evaluated in this study did not show substantial statistical differences.
In a recent study,
Aly and colleagues [16] support this affirmation.
Fig. 17 Fig. 18
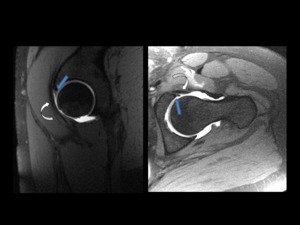
Fig. 18: A 35-years-old woman with left groin pain, especially with the supine and sitting position, nonspecific focal tenderness over the iliopsoas tendon area and a positive impingement test.
No radiographic hallmarks of femoroacetabular impingement were presents (not shown).
Sagittal and axial oblique T1 fat saturated MR arthrographic images of left hip show a small anterior labral tear (blue arrow) directly beneath the iliopsoas tendón (curved white arrow).
This combination of clinical and radiological findings is suggestive of iliopsoas impingement.
References: References: Radiology, Unidad Central de Radiodiagnóstico, Hospital Infanta Leonor - Madrid/ES
In any case,
further research is needed to examine pathologic mechanisms,
to establish a causal relationship between abnormalities of the iliopsoas tendon and labral damage and to validate possible radiologic criteria.
[1,3]
-Treatment
Surgical management of iliopsoas impingement includes labral debridement or repair combined with tenotomy of the iliopsoas tendon at the level of the acetabulum.
[14,15]
Suggesting this diagnosis preoperatively can be very helpful because this condition may go unrecognized at time of hip arthroscopy if it is not suspected.

 in the ischiofemoral space. The QFM is a flat and quadrilateral shaped muscle located between the ischial tuberosity medially and femoral lesser trochanter laterally (crossed lines). It arises from the upper part of the lateral border of the ischial tuberosity, just anterior to the hamstring tendon origin (bordered by the yellow line), and inserts at the intertrochanteric crest on the posterior aspect of the proximal femur. Anteriorly, the QFM is bordered by the obturator externus muscle (star) and posteriorly it is bordered by fat and the sciatic nerve (blue arrow). References: References: Radiology, Unidad Central de Radiodiagnóstico, Hospital Infanta Leonor - Madrid/ES")
 and quadratus femoris space (QFS-red line). References: References: Radiology, Unidad Central de Radiodiagnóstico, Hospital Infanta Leonor - Madrid/ES")
.
Axial proton density-weighted fat-suppressed MR image of the same patient shows edema within QFM(curved arrow)and subcortical cystic changes with edema in the ischial tuberosity (thin blue arrow). References: References: Radiology, Unidad Central de Radiodiagnóstico, Hospital Infanta Leonor - Madrid/ES")
 demostrate ischiofemoral impingement in left hip with narrowed IFS(blue line in CT), diffuse edema with moderate fatty infiltration of QFM (curved arrow) and mass effect of QFM on sciatic nerve(blue arrow). References: References: Radiology, Unidad Central de Radiodiagnóstico, Hospital Infanta Leonor - Madrid/ES")
, mass effect of QFM on sciatic nerve (white circle) and tendinopathy of hamstring tendons(red arrow).
Mild edema and fatty infiltration of left QFM is also noted. References: References: Radiology, Unidad Central de Radiodiagnóstico, Hospital Infanta Leonor - Madrid/ES")
;QFS narrowed and mild edema of QFM in the left hip is also noted. References: References: Radiology, Unidad Central de Radiodiagnóstico, Hospital Infanta Leonor - Madrid/ES")
 and severe fatty infiltration of QFM in both hips. Mild QFM edema (curved arrow) and mild tendinopathy of hamstring tendons (red arrow) is also noted in the right hip. References: References: Radiology, Unidad Central de Radiodiagnóstico, Hospital Infanta Leonor - Madrid/ES")
, just above the anterosuperior acetabular rim (red line) with normal appearance. References: References: Radiology, Unidad Central de Radiodiagnóstico, Hospital Infanta Leonor - Madrid/ES")
 between the caudad level of the AIIS (blue arrow) and the anterosuperior acetabular rim in both hips. Type I AIIS variant. References: References: Radiology, Unidad Central de Radiodiagnóstico, Hospital Infanta Leonor - Madrid/ES")
 sit just at the level of the acetabular rim (red arrow) and appears as a ‘‘rooflike’’ prominence over the hip. Type II AIIS variant. References: References: Radiology, Unidad Central de Radiodiagnóstico, Hospital Infanta Leonor - Madrid/ES")
 in the right hip extending caudad to the level of the anteriorsuperior acetabular rim (red arrow). Type III AIIS variant. References: References: Radiology, Unidad Central de Radiodiagnóstico, Hospital Infanta Leonor - Madrid/ES")
.
Anteroposterior pelvis radiographs, 3D CT reconstruction and coronal T1-weighted MR images demonstrate prior avulsion injury of the AIIS with secondary deformity and bony hypertrophy (blue arrow), extending caudad to the level of the anteriorsuperior acetabular rim (type III variant). He was diagnosed with subspine impingement in the right hip.
Note that on left side, AIIS is slightly enlarged after prior similar injury (red arrow), but osseous protrusion is smaller (type II variant). References: References: Radiology, Unidad Central de Radiodiagnóstico, Hospital Infanta Leonor - Madrid/ES")
. Patients was able to return to training and competition at 6 months after the surgery. References: References: Radiology, Unidad Central de Radiodiagnóstico, Hospital Infanta Leonor - Madrid/ES")
 with bony hypertrophy protruding inferiorly below the level of the anteriorsuperior acetabular rim (red line in sagittal view) (type III variant). She was diagnosed with subspine impingement in right hip. On left side, the AIIS is slightly enlarged after similar injury, but osseous protrusion (red arrow) is much smaller (type II variant). References: References: Radiology, Unidad Central de Radiodiagnóstico, Hospital Infanta Leonor - Madrid/ES")
 very close to the AIIS, representing calcified deposits within the rectus femoris tendon as a result of old injury. References: References: Radiology, Unidad Central de Radiodiagnóstico, Hospital Infanta Leonor - Madrid/ES")
. The transverse acetabular ligament (red arrow) is define as 6 o´clock (inferior). References: References: Radiology, Unidad Central de Radiodiagnóstico, Hospital Infanta Leonor - Madrid/ES")
.
Axial oblique and sagittal T1 fat saturated MR arthrographic images of right hip demonstrate a small localized anterior labral tear (blue arrow)at 3 o'clock position, directly adjacent to iliopsoas tendón (curved white arrow).
This combination of clinical and radiologic findings is suggestive of iliopsoas impingement. References: References: Radiology, Unidad Central de Radiodiagnóstico, Hospital Infanta Leonor - Madrid/ES")
.
Sagittal and axial oblique T1 fat saturated MR arthrographic images of left hip show a small anterior labral tear (blue arrow) directly beneath the iliopsoas tendón (curved white arrow).
This combination of clinical and radiological findings is suggestive of iliopsoas impingement. References: References: Radiology, Unidad Central de Radiodiagnóstico, Hospital Infanta Leonor - Madrid/ES")