Methods and materials
65 lesions in 62 patients (women,
28-80,
mean 56 years) with invasive breast cancer were enrolled for this study,
who were treated with neoadjuvant chemotherapy and underwent dynamic MR imaging before mastectomy from July 2011 to April 2014.
All lesions were biopsied and diagnosed as invasive breast cancer before the therapy.
Regimens of neoadjuvant chemotherapy
Weekly paclitaxel + trastuzumab → FEC; 28 patients
Weekly paclitaxel → FEC; 17 patients
FEC → weekly paclitaxel; 4 patients
Others; 13 patients
(Note.
FEC: 5-fluorouracil + epirubicin + cyclophosphamide)
The regimen was not fixed in this series.
Chemotherapy with weekly paclitaxel with or without trastuzumab followed by FEC was performed in more than half of the patients.
Standard doses
Paclitaxel 80 mg/m2
Epirubicin 100 mg/m2
5-fluorouracil 500 mg/m2
Cyclophosphamide 500 mg/m2
Dose was reduced based on the status of patients.
Dynamic MR imaging protocol
Philips Achieva 1.5T scanner
SENSE-breast-7ch receiver coil
0.2 mL/KgBW of Gd-DTPA or gadodiamide was administrated at a rate of 2 mL/sec.
Scanning was initiated at the start of injection.
Dynamic study was performed with serial bilateral axial imaging of a scanning time of 1 min.
Unilateral high-resolution sagittal scanning was intercalated at the tumor side and contralateral side during a delayed phase.
e-THRIVE with SPAIR,
TR 6.3 or 6.6,
TE 3.1 or 3.2,
flip angle 10° was used.
SENSE technique of a factor 2.7 was applied for bilateral axial scanning.
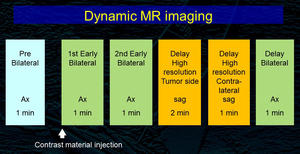
Fig. 1: Dynamic MR imaging protocol
Image review
A radiologist reviewed MR images in a blind manner and studied the presence or absence,
enhancement patterns and time intensity curves (TIC) of residual disease according to BI-RADS-MRI 2013.
No visualization of contrast enhancement was considered as no residual disease (complete response) and the depiction was considered as the presence of viable residual disease.
The results were correlated with the pathological findings.

