Clinical Features
Risk factors
1. Ethnicity,
gender,
and age
Primary carcinoma of the gallbladder is an uncommon though aggressive malignancy with marked ethnic and geographical variations.
Worldwide,
gallbladder cancer has a low occurrence <2 per 100,000,
but has a wide variance.
Gallbladder cancer is rare in developed countries.
In the U.S.,
it accounts for less than 5,000 cases per year (1).
High rates of gallbladder carcinoma are seen in South American countries,
particularly Chile,
Bolivia,
and Ecuador,
as well as some areas of India,
Pakistan,
Japan and Korea.
In Chile,
mortality rates from gallbladder carcinoma are the highest in the world (2).
Sex – Women are affected two to six times more often than men. Worldwide there is marked predominance of women over men,
especially in northern India,
Pakistan,
and in American Indian females (3).
Age – Gallbladder cancer rates tend to increase with advancing age.
In a Memorial Sloan-Kettering report of 435 gallbladder cancer patients the median age at presentation was 67 years (4).
2. Cholelithiasis
Cholelithiasis is a well established risk factor for the development of gallbladder carcinoma and gallstones are present in approximately 85% of affected patients (2) (Figure 2).
Further,
gallbladder cancer rates correlate well with the prevalence of gallstone disease,
however the overall risk of gallbladder cancer in patients with cholelithiasis is low; less than 3% case of cholelithiasis have gall bladder carcinoma (2).
The basis for this relationship likely resides in gallstones causing chronic irritation and inflammation of the gallbladder,
perhaps aided by the local production of carcinogens,
such as secondary bile acids which leads to mucosal dysplasia and subsequent carcinoma (5).
Gallstone characteristics further influence the frequency of gallbladder cancer.
Increasing stone size augments the risk of gallbladder cancer; stones >3 cm have a tenfold increased risk (6).
The stone type may also matter; high prevalence of cholesterol gallstone disease is found to be associated with high incidence of gallbladder cancer in American Indians and other groups (7).
In support of this association,
an inverse correlation exists between cholecystectomy for cholelithiasis and gallbladder cancer rates (5).
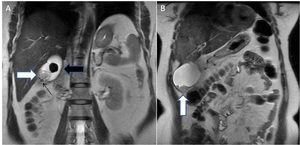
Fig. 2: (A & B) 45 year old female patient complaining of pain upper abdomen; Coronal T2W MR images reveal: A large T2 hypointense (thick black arrow) and multiple small (thin black arrow) intraluminal gallbladder calculi with eccentric polypoidal soft tissue mass in fundal region (white arrow).
3. Chronic inflammation
Chronic inflammation is implacably linked to malignant transformation,
being a major factor in carcinogenesis.
Recurrent or chronic inflammatory insults are detrimental,
causing DNA damage and release of inflammatory mediators,
and thus,
predisposing cells to oncogenic transformation (2).
Hence,
cholelithiasis with its attendant repeated trauma,
resulting in chronic cholecystitis,
might be the mechamism for cancer development after many years.
Chronic inflammation can also result in calcium deposition in the gallbladder wall.
Porcelain gallbladder is an uncommon condition (<1% of gallbladder specimens) with extensive wall calcification (Figure 3),
which also appears to be associated with gallbladder carcinoma in 12%-61% of patients (8).
Gallbladders with partial calcification,
stippled,
or multiple punctuate calcifications in the glandular spaces of the mucosa should be removed prophylactically (6); cases exhibiting transmural calcification are less likely to be associated with carcinoma (8).
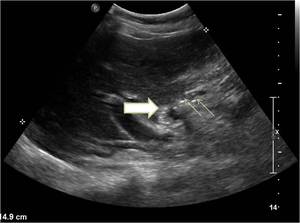
Fig. 3: Porcelain gallbladder. Ultrasound image showing contracted gallbladder with mural calcification (thick white arrow) and multiple small intraluminal calculi (thin white arrow).
4. Infections
Chronic bacterial cholangitis constitute a clear risk for biliary tract malignancy.
The organisms most implicated are Salmonella and Helicobacter (9).
Some 6% of typhoid carriers develop gallbladder cancer; with a 12 fold increased risk.
5. Primary sclerosing cholangitis
There is an increased frequency of gallbladder mass lesions in patients with PSC; presumably related to the ongoing inflammation,
facilitating a metaplasia-dysplasia-carcinoma sequence (10).
6. Exposures
Various environmental exposures have been hypothesized to contribute to gallbladder cancer.
Tobacco is a significant risk factor.
Heavy metals,
like nickel and cadmium,
have been implicated including,
drugs like methyldopa and isoniazid (11).
Radon,
an inhaled gas has also been associated with cancer of the lung and gallbladder (12).
7. Obesity
Obese people (body mass index [BMI] >30 kg/m2) have an increased risk of developing gallbladder cancer.
For each 5-point increase in BMI,
the relative risk of developing gallbladder cancer increases by 1.59 for women and 1.09 for men (13).
8. Gallbladder polyps
Gallbladder polyps seen in almost 5% of adults are mostly pseudopolyps,
without neoplastic potential,
as: cholesterol polyps (~60% of all gallbladder polyps); adenomyosis (~25%); or inflammatory polyps (~10%) (Figure 4A,B).
The features of polypoidal masses that indicate malignancy include: large polyps (>1 cm; 25% being malignant); a solitary polyp; a sessile polyp; polyp growth; assosciated gallstones; and age over 50-60 years (14) (Figure 4C,D).
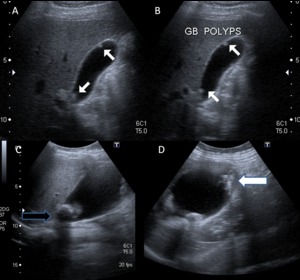
Fig. 4: Benign and malignant polyp. (A,B) Ultrasound depicting multiple small (<1 cm) echogenic polyps (white arrow) along non-dependant wall of gallbladder - likely benign. (C,D) Another case displaying large irregular polypoidal soft tissue thickening in gallbladder fundal region (white arrow) with cholelithiasis (black arrow) on USG; postcholecystectomy histopathological examination revealed adenocarcinoma
9. Anomalous pancreaticobiliary junction
This is a congenital malformation in which the pancreatic duct drains into the biliary tract outside the duodenal wall,
potentially allowing pancreatic secretions to regurgitate into the bile ducts and gallbladder,
leading to malignant changes in the mucosa (2).
Approximately 10% of patients with gallbladder cancer have this anomaly; manifesting histologically as a papillary carcinoma (3).
10.
Genetics
Carcinoma of the gallbladder is likely a multistep sequence involving cumulative genetic and epigenetic alterations (2).
A family history of gallbladder disease increases the risk of developing gallbladder cancer,
and the genetic background accounts for approximately 25% of the total gallstone disease risk (15).
Clinical Diagnosis
The diagnosis of gallbladder carcinoma is usually unsuspected in early stages and is typically diagnosed incidentally because of inflammatory symptoms related to coexistent cholelithiasis or cholecystitis.
About one percent of patients undergoing cholecystectomy for cholelithiasis have an incidental gallbladder carcinoma (16).
The majority of patients with gallbladder carcinoma present with advanced disease.
Chronic abdominal pain,
anorexia,
or weight loss are common initial symptoms (17).
Jaundice usually presents as a result of malignant obstruction of the biliary tree rather than hepatic metastasis or coexistent choledocholithiasis (18).
Physical examination may demonstrate a palpable mass,
hepatomegaly and jaundice.
Elevated serum levels of α-fetoprotein and carcinoembryonic antigen have been reported in association with gallbladder carcinoma (19).
Pathological features
Histological features
The normal gallbladder wall is composed of four layers: mucosa,
lamina propria,
an irregular muscle layer,
and connective tissue (Fig.5).
The surface epithelium is composed of a single layer of columnar epithelium with basal nuclei and eosin-ophilic cytoplasm.
There is no muscularis mucosa or submucosa.
Along the hepatic surface,
the connective tissue is continuous with the interlobular connective tissue of the liver.
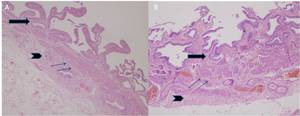
Fig. 5: Normal gallbladder. (A,B) Photomicrograph [2X (A) and 40X(B); hematoxylin-eosin stain] shows the mucosa as a single layer of columnar epithelium with underlying lamina propria (thick arrows), irregular muscle layer (thin arrows), and connective tissue (arrowheads).
- Gallbladder carcinomas are epithelial in origin and account for 98% of all gallbladder malignancies.
- The remainders are sarcomas,
lymphomas,
carcinoid,
metastases,
and other unusual malignancies.
- Adenocarcinomas account for 90% of gallbladder carcinomas and are characterized by glands lined by cuboidal or columnar cells,
which may contain mucin.
They may be well,
moderately,
or poorly differentiated.
There are several recognized histologic variants of adenocarcinoma: papillary,
intestinal,
mucinous,
signet-ring cell,
and clear cell (20).
Many tumors contain more than one histologic variant.
- The papillary adenocarcinoma consists of branching fibrovascular stalks lined by atypical cuboidal or columnar cells (Fig.6).
Papillary carcinomas tend to fill the lumen of the gallbladder before invading the gallbladder wall; therefore,
they are associated with a better prognosis than other variants (21).
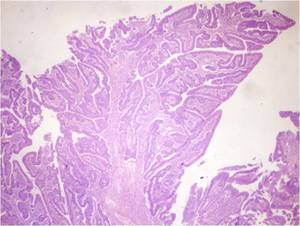
Fig. 6: Papillary carcinoma. Photomicrograph (200X; hematoxylin-eosin stain) showing branching fibrovascular stalks lined by atypical cuboidal or columnar cells.
- The intestinal type adenocarcinoma resembles intestinal epithelium and is believed to be a variant of well-differentiated adenocarcinoma.
This category has two subtypes,
which are characterized by the appearance of the intestinal glands: (a) those lined chiefly by goblet cells and
(b) those resembling the glands of colonic adenocarcinoma (22).
- Mucinous adenocarcinomas are those tumors that consist of more than 50% extracellular mucin (20).
There are two histologic variants: one contains large pools of extracellular mucin with small clusters of malignant epithelial cells,
and the other is characterized by mucin-filled glands with cystic dilatation.
- Signet-ring cell carcinoma contains cells with abundant intracytoplasmic mucin,
which displaces the nuclei to the periphery (Fig.
7).
Infiltrative submucosal growth can be a prominent feature of signet-ring cell tumors and may occasionally resemble linitis plastica of the stomach.
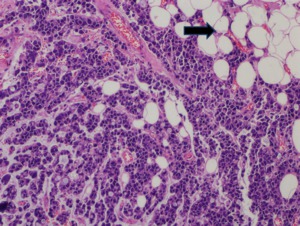
Fig. 7: Signet-ring cell carcinoma. Photomicrograph (200X; hematoxylin-eosin stain) shows neoplastic epithelial cells with abundant intracytoplasmic mucin, which displaces the nuclei to the periphery (arrow).
- Clear cell adenocarcinoma of the gallbladder is composed of cords,
sheets,
nests,
and trabeculae of clear cells with well-defined cytoplasmic borders (23) and may be confused histologically with metastatic renal cell carcinoma.
However,
clear cell adenocarcinomas may also contain areas mixed with conventional adenocarcinoma and mucin production; findings that help distinguish these tumors from renal cell carcinoma.
- The remaining epithelial cell types occurring in the gallbladder include adenosquamous carcinoma,
squamous cell carcinoma,
small (oat) cell carcinoma,
and undifferentiated carcinoma.The adenosquamous carcinoma contains a mixture of malignant glandular and squamous components.
The pure squamous cell carcinoma constitutes only 1% of all malignant gallbladder tumors and consists of cords,
islands,
or sheets of malignant squamous cells separated by dense fibrous stroma (22) (Fig.
8).
Small (oat) cell carcinomas of the gallbladder are rare and highly aggressive tumors.
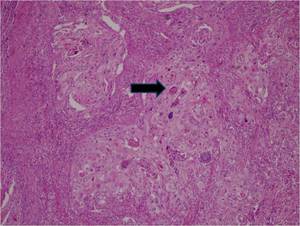
Fig. 8: Squamous cell carcinoma. Photomicrograph (100X; hematoxylin-eosin stain) shows nests of well-differentiated, neoplastic, keratinizing squamous cells (arrow) that infiltrate the gallbladder wall.
- Paraneoplastic syndromes may be associated with small cell carcinoma of the gallbladder,
and Cushing syndrome has been reported in association with a corticotropin-secreting apudoma of the gallbladder (24).
Gross Pathologic Features
- The majority (68%) of gallbladder carcinomas are diffusely infiltrating lesions,
and the remainder exhibit intraluminal polypoid growth (32%) (25).
- Approximately 60% of tumors originate in the gallbladder fundus,
30% in the body,
and 10% in the neck (22).
- Submucosal spread of infiltrating carcinomas appears grossly as focal or diffuse areas of wall thickening (Fig.
9),
nodularity,
or induration in the gallbladder wall.

Fig. 9: Well differentiated adenocarcinoma. Photograph of a resected gallbladder (cut specimen) shows focal neoplastic mural thickening involving the body and neck region of gallbladder(arrow). Scale is in centimeters
- In some cases of direct invasion,
a thick neoplastic wall encases the gallbladder when direct extension to the liver has occurred (22).
- The less common papillary adenocarcinomas exhibit intraluminal polypoid growth.
This tumor is usually sessile and has a cauliflower-like appearance (22).
Radiological features
Radiologic Evaluation of the Primary Tumor
Imaging modalities used in evaluating gallbladder diseases include ultrasonography,
endoscopic ultrasonography,
computer tomography,
and MRI (26).
Gallbladder carcinoma may appear at any of these imaging modalities as (Fig.1):
1.
Mass occupying or replacing lumen (40-60%)
2. Focal or diffuse gallbladder wall thickening (20-30%).
3. Intraluminal polypoid mass (15-25%)

Fig. 1: Pictorial diagram displaying three different types of imaging menifestations of carcinoma gallbladder as (1)a mass replacing the normal gallbladder, (2)diffuse or focal thickening of the gallbladder wall, (3) or a polypoid mass within the gallbladder lumen.
1.
Mass occupying or replacing lumen
Gallbladder carcinoma most commonly presents as a large mass that nearly fills or replaces the gallbladder lumen,
often directly invading the surrounding liver parenchyma.
At ultrasonography (US), irregularly marginated,
heterogenous predominantly hypoechoic mass fills much or all of the gallbladder lumen.
Heterogeneous echotexture reflects varying degrees of tumor necrosis with anechoic areas of trapped bile.
Echogenic foci and acoustic shadowing associated with the tumor may represent coexisting gallstones (Fig.
10),
gallbladder wall calcification,
or tumoral calcification (27).
Direct extension to the liver and biliary tree is a common associated finding with large,
advanced carcinomas.
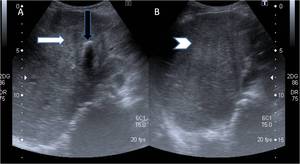
Fig. 10: (A&B) Ultrasound images showing a large illmarginated heterogeneously hypo-echoic mass lesion replacing gallbladder (arrow) with adjacent hepatic infiltration (arrowhead). Note echogenic focus with distal acoustic shadowing within the mass lesion suggestive of calculi (black arrow).
Contrast enhanced CT may demonstrate a hypoattenuating or isoattenuating mass in the gallbladder fossa and hepatic infiltration with protrusion of the anterior surface of the left lobe medial segment (28)(Fig.
11).
The tumor mass may contain low-attenuation areas of necrosis.
Areas of enhancement reflect viable tumor (29).
Biliary obstruction at the level of the porta hepatis and lymph node metastasis are frequent associated finding (30).
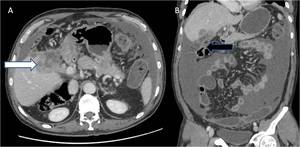
Fig. 11: (A & B) Axial and coronal contrast enhanced CT images showing heterogeneously enhancing lobulated soft tissue mass lesion replacing gallbladder with adjacent hepatic (white arrow) and colonic (hepatic flexure) infiltration (black arrow). In addition, moderate ascites is also noted.
On MRI, gallbladder carcinoma usually shows hypo- to isointense signal characteristics on T1-weighted and moderately hyperintense signal characteristics on T2-weighted sequences (30).
2.
Focal or diffuse asymmetric gallbladder wall thickening
Wall thickening is the most diagnostically challenging of the three patterns because it mimics the appearance of more common acute and chronic inflammatory conditions of the gallbladder (30).
Subtle areas of wall thickening may reflect early carcinomas however,
they are difficult to detect on imaging.
Pronounced wall thickening (ie,
>1.0 cm) demonstrated by US (Fig.
12) or CT (31),
with associated mural irregularity or marked asymmetry should raise concerns for malignancy or complicated cholecystitis (32).
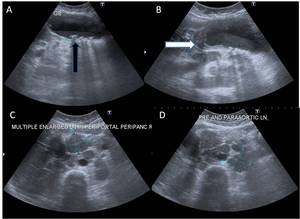
Fig. 12: (A-D)In a known case of cholelithiasis, ultrasound images reveal: (A)distended gallbladder with multiple intraluminal calculi (black arrow)and layering of sludge, (B)annular mural thickening in neck region of gallbladder (white arrow) with, (C) periportal/peripancreatic and (D) pre/paraaortic lymphadenopathy.
Contrast-enhanced CT with dual phase technique showing differential gallbladder wall enhancement is extremely helpful for distinguishing between benign and malignant causes of gallbladder wall thickening.
MDCT findings of hyper enhancing thick inner wall ≥ 2.6 mm during the portal venous phase,
weakly enhancing or nonenhancing thin outer wall ≤ 3.4 mm,
and irregular and focal wall thickening indicate a malignant cause of flat gallbladder wall thickening rather than benign disease (33).
The CT demonstration of associated lymphadenopathy (Fig.
13),
soft-tissue extension into the liver,
and evidence of hematogenous metastases favors the diagnosis of gallbladder carcinoma.
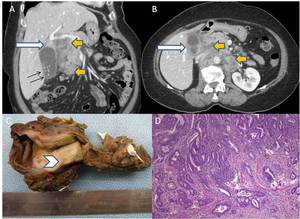
Fig. 13: (A-D) Same patient underwent contrast enhanced CT and radical cholecystectomy with lymph node dissection: (A,B) Coronal and axial CT images reveal cholelithiasis (black arrow) with annular mural thickening in gallbladder neck region (white arrows) and periportal/peripancreatic, pre/para-aortic lymphadenopathy (yellow arrows) (C) Photograph of resected gallbladder (cut specimen) shows focal neoplastic mural thickening involving the body and neck region of gallbladder(arrowhead) (D) Photomicrograph(10X; HE stain) revealed well differentiated adenocarcinoma of gallbladder.
Magnetic resonance (MR) imaging although is typically not employed as a primary imaging modality for the gallbladder,
it may be useful in cases of focal or diffuse mural thickening to distinguish gallbladder carcinoma from adenomyomatosis and chronic cholecystitis (30).
The endoscopic ultrasonography is also found to be effective in the diagnosis of gallbladder carcinoma and determination of the extent of tumor invasion (34) with greater accuracy by contrast enhanced endosonography(35).
Real-time elastography using acoustic radiation force impulse (ARFI) is a new emerging technique,
which has also been shown to differentiate between benign and malignant nodules in various organs (36).
At a cut-off value of 2.7 m/s,
elastography showed overall accuracy of 92.8% with sensitivity and specificity of 100% and 91.3%,
respectively,
for diagnosing gallbladder carcinoma (37).
3.
Intraluminal polypoid mass
The less common intraluminal polypoid carcinoma may exhibit a well-defined,
round or oval shape on cross-sectional images.
Sonographically demonstrating immobility of intraluminal mass with changes in patient position allows distinction of tumor mass from tumefactive sludge (38).
CT - The tumor may be hypoattenuating or isoattenuating and subtle extension of the tumor beyond the gallbladder wall may be better depicted on CT.
MR Imaging demonstrates prolongation of the T1 and T2 relaxation times (Fig.
14) and ill-defined early enhancement at dynamic gadolinium-enhanced MR imaging is a typical appearance of these tumors (39).
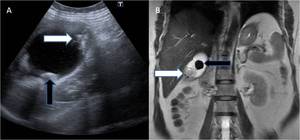
Fig. 14: (A,B) A 56 year old lady presented with pain abdomen; (A) Ultrasonography revealed cholelithiasis (black arrow) with polypoidal soft tissue thickening in gallbladder fundal region (white arrow), Subsequently MRI confirmed polypoidal mass in fundus of gallbladder displaying T2 hyperintensity on coronal T2WI (B). Later cholecystectomy was performed and histopathological examination revealed mucinous adenocarcinoma.
Radiologic Evaluation of Tumor Extension
Modes of spread of gallbladder carcinoma to adjacent organs:
1. Direct extension is the most common.
Contiguous spread of tumor is facilitated by the thin gallbladder wall,
which lacks a substantial lamina propria and has only a single muscular layer.
In addition,
the perimuscular connective tissue of the gallbladder is continuous with the interlobular connective tissue of the liver (40).
- The liver is most frequently involved by direct contiguous spread (65% of cases),
followed by the colon (15%),
duodenum (15%),
and pancreas (6%) (41) (fig.
15).
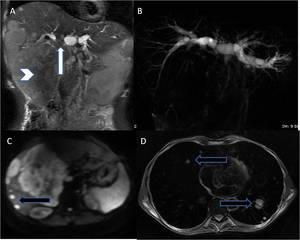
Fig. 15: (A-D) Case of advanced carcinoma of gallbladder; (A,B) Coronal T2WI and thick slab 2D MRCP images reveal large mass replacing gallbladder with surrounding hepatic infiltration (arrowhead) and extension to hilar region (white arrow) with resultant hilar block and attendant moderate upstream biliary dilatation. (C,D) DWI and axial T2WI reveal hepatic and pulmonary metastases(black arrows).
- Infiltrative tumor may spread along the cystic duct to the extrahepatic bile duct,
and intraductal spread of tumor results in biliary dilatation and obstruction (fig.
16).
Biliary dilatation is a common finding in gallbladder carcinoma,
occurring in 38% of patients in one series (42).
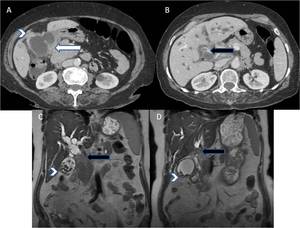
Fig. 16: (A-D) A case of locally advanced carcinoma of gallbladder; (A,B) Contrast enhanced axial CT and (C,D)coronal T2W MR images reveal diffuse asymmetric circumferential mural thickening of gallbladder (white arrows) with adjacent hepatic (arrowhead) and duodenal infiltration (white arrow) and contiguous extension along cystic duct to involve proximal third of common duct (black arrow) and resultant upstream biliary dilatation.
2. Lymphatic - The prevalence of lymphatic spread is high in gallbladder carcinoma.
Lymphatic metastases progress from the gallbladder fossa through the hepatoduodenal ligament to nodal stations near the head of the pancreas.
Three pathways of lymphatic drainage have been suggested (43): - i)cholecystoretropancreatic pathway,
ii)cholecystoceliac pathway,
iii)cholecystomesenteric pathway
The cystic and pericholedochal lymph nodes are the most commonly involved at surgery (44) and are a critical pathway to involvement of the celiac,
superior mesenteric and para-aortic lymph nodes.
The node of the foramen of Winslow,
the superior pancreatoduodenal node,
and the posterior pancreatoduodenal nodes are the most common nodes demonstrated by CT (45).
Positive lymph nodes are more likely to be greater than 10 mm in anteroposterior dimension and have ring like or heterogeneous contrast material enhancement (46) (Fig.
17).
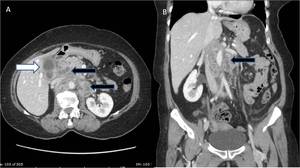
Fig. 17: (A,B) A case of carcinoma gallbladder; contrast enhanced (A) axial and (B) coronal sections of abdomen reveals, annular asymmetric mural thickening of gallbladder with adjacent hepatic infiltration (white arrow) and characteristic enlarged (>10mm), ring enhancing pancreatoduodenal, para-aortic and superior mesenteric lymphnodes (black arrows).
3. Vascular- Hematogenous metastases are most commonly seen in the liver (41) (Fig.
18A).
Pulmonary (Fig.
18B),
skeletal,
cardiac,
pancreatic,
renal,
adrenal,
and cerebral metastases occur less frequently.

Fig. 18: (A,B) A case of carcinoma gallbladder; contrast enhanced axial sections of (A) abdomen and (B) chest reveals, annular asymmetric mural thickening of gallbladder with adjacent hepatic infiltration (white arrow) and hepatic and pulmonary metastases (black arrows).
4. Intraperitoneal (Fig.
19)
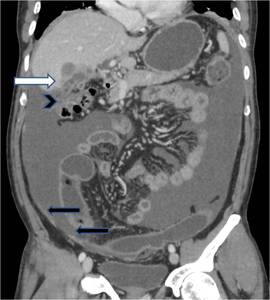
Fig. 19: Coronal reformatted contrast enhanced CT image reveals, heterogeneously enhancing mass in gallbladder fossa region (white arrow) with surrounding mesenteric fat stranding in subhepatic region and adjacent colonic infiltration (arrowhead) with moderate ascites and nodular enhancing peritoneal thickening (black arrows) in keeping with intraperitoneal spread of carcinoma gallbladder.
5. Intraductal
6. Neural
- Barium enema study and an upper gastrointestinal series may demonstrate the findings of adjacent bowel invasion.
- Extension of the primary tumor into the liver or hepatoduodenal ligament is well depicted by CT and MR imaging.
- Hematogenous metastases to the liver are also well depicted by CT and MR imaging.
- Direct cholangiography (endoscopic retrograde cholangiopancreatography [ERCP],
percutaneous transhepatic cholangiography,
or intraoperative cholangiography) may be performed in cases with biliary involvement when the diagnosis of gallbladder carcinoma is unsuspected or when therapeutic management of biliary obstruction is necessary (Fig.
20).
Cholangiography may demonstrate malignant strictures or obstruction involving the extrahepatic bile ducts,
confluence of the right and left hepatic ducts,
and right lobe intrahepatic ducts (47).
Associated findings from cholangiography include intraluminal gallbladder filling defects that may represent tumor or stones,
a mass displacing and invading the gallbladder,
and intraductal filling defects that may represent tumor or coexistent choledocholithiasis.
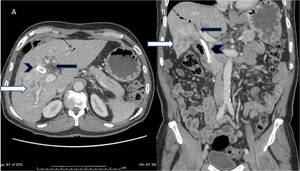
Fig. 20: (A,B) Axial and coronal reformatted contrast enhanced CT images; A case of advanced carcinoma gallbladder with hepatic infiltration (white arrows) and hilar block (black arrows) with PTBD sent (arrowheads) and pneumobilia (thin black arrows).
Staging
The TNM [ Fig. 21 (Table 1) and Fig. 22 (Table 2)] (48) and modified Nevin [ Fig. 23 (Table 3) (49)] classifications are used for staging gallbladder carcinoma.
Role of US
- Useful for detecting the primary tumor and adjacent liver invasion,
but cannot reliably depict the full extent of disease.
- Bach et al (50) showed that only 37% of patients with advanced disease were identified with US.
- In addition,
the potentially curable stage 1 cancers are difficult to detect sonographically (51).
- Several authors have reported the successful use of endoscopic US for evaluating the depth of gallbladder carcinoma invasion (52).
Role of CT
- More useful than US for detecting lymph node involvement,
adjacent organ invasion,
and distant metastasis.
- CT does not reliably demonstrate all regional lymph nodes,
but,
when abnormally sized nodes (>10 mm) are present,
it does indicate lymphatic spread (46).
In a retrospective study of 59 patients,
the sensitivity of CT in the detection of abnormal lymph nodes was 36% for N1 nodes and 47% for N2 nodes; CT had a specificity of 99% for both N1 and N2 nodes (53).
In the same study,
CT had a sensitivity of 100% in the detection of tumor extension greater than 2 cm into the liver (T4 stage); however,
its sensitivity in the detection of less severe tumor extension into the liver (<2 cm or T3 stage) was only 65% (53).
Radiologic differential diagnosis
Gallbladder carcinoma manifesting as diffuse gallbladder wall thickening has a differential diagnosis that includes:
- Inflammatory and noninflammatory causes of wall thickening.
These conditions include heart failure,
cirrhosis,
hepatitis,
hypoalbuminemia,
renal failure,
and cholecystitis (Fig.
24).
Gallbladder carcinoma should be suspected when there are features of a focal mass,
lymphadenopathy,
hepatic metastases,
and biliary obstruction at the level of the porta hepatis (54).
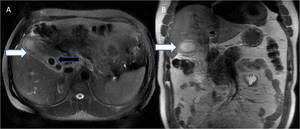
Fig. 24: Acute calculus cholecystitis. 40 year old lady complaining of severe pain abdomen; (A) Axial and (B) Coronal T2W MR images reveal diffuse symmetric T2 hyperintense gallbladder wall thickening (white arrows) with T2 hypointense intraluminal calculi (black arrow) and mild pericholecystic fat stranding.
- Xanthogranulomatous cholecystitis is a pseudotumoral inflammatory condition of the gallbladder that radiologically simulates gallbladder carcinoma (52).
The CT features of xanthogranulomatous cholecystitis and gallbladder carcinoma overlap substantially (Fig.
25); thus,
these entities cannot be reliably differentiated (55).
Both diseases may demonstrate gallbladder wall thickening,
infiltration of the surrounding fat,
hepatic involvement,
and lymphadenopathy.
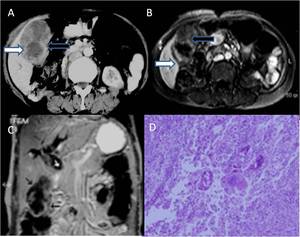
Fig. 25: Xanthogranulomatous cholecystitis. (A) Axial contrast enhanced CT and (B) Axial post contrast T1W MR images reveal heterogeneously enhancing lobulated gallbladder wall thickening (white arrows) with poorly enhancing intramural areas (black arrows). (C) Coronal MR images reveal attendant biliary dilatation (small white arrows). (D) High power view showing dense inflammation comprising of foamy macrophages, lymphocytes, neutrophils & foreign body type of giant cells.
References: Images reproduced from: Arora A, Puri SK, Upreti L, Kapoor A, Vandana. Xanthogranulomatous cholecystitis masquerading as gallbladder carcinoma, {Online}. DOI: 10.1594/EURORAD/CASE.8648
- Adenomyomatosis is a common tumorlike lesion of the gallbladder with no malignant potential (22).
It may involve the gallbladder in a focal,
segmental,
or diffuse form.
Its histologic features include a proliferation of epithelial and mural elements,
and Rokitansky-Aschoff sinuses are seen as prominent infoldings of the epithelium (Fig.
26).
At US,
adenomyomatosis is characterized by focal or diffuse gallbladder wall thickening and anechoic or echogenic foci in the gallbladder wall (56).
These echogenic foci may produce a ring-down reverberation artifact.
Rokitansky-Aschoff sinuses are best visualized with MR imaging performed with breath-hold technique and T2-weighted pulse sequences (57); therefore,
MR imaging can be useful for distinguishing this benign entity from gallbladder carcinoma.
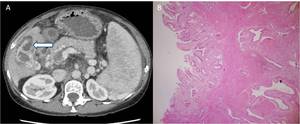
Fig. 26: GB Adenomyomatosis. (A) Axial contrast enhanced CT images reveal diffuse gallbladder wall thickening with intramural cystic spaces. Note is made of cirrhotic liver architecture with splenomegaly , multiple abdominal collaterals and portal vein thrombosis. (B) Photomicrograph (40X;HE stain) shows glands in the muscle layer with stroma- Adenomyomatous changes.
The differential diagnosis for those tumors that manifest as an intraluminal polypoid mass includes adenomatous,
hyperplastic,
and cholesterol polyps (Fig.
27); carcinoid tumor; metastatic melanoma; and a hematoma within the gallbladder.
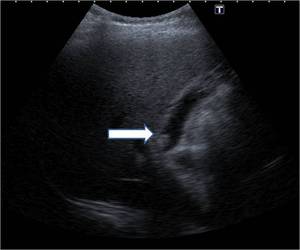
Fig. 27: Ultrasound image showing polyp in neck region of gallbladder(arrow).
The differential diagnosis for a mass replacing the gallbladder fossa includes hepatocellular carcinoma,
cholangiocarcinoma (Fig.
28),
and metastatic disease to the gallbladder fossa.
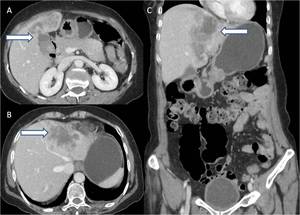
Fig. 28: (A,B) Axial contrast enhanced CT and (C) coronal reformatted images reveal lobulated heterogeneously enhancing mass lesion involving left lobe of liver (arrows) in close proximity to gallbladder. Differentials include mass forming intrahepatic cholangiocarcinoma and carcinoma gallbladder with hepatic infiltration.

a mass replacing the normal gallbladder, (2)diffuse or focal thickening of the gallbladder wall, (3) or a polypoid mass within the gallbladder lumen.")
 45 year old female patient complaining of pain upper abdomen; Coronal T2W MR images reveal: A large T2 hypointense (thick black arrow) and multiple small (thin black arrow) intraluminal gallbladder calculi with eccentric polypoidal soft tissue mass in fundal region (white arrow).")
 and multiple small intraluminal calculi (thin white arrow).")
 Ultrasound depicting multiple small (<1 cm) echogenic polyps (white arrow) along non-dependant wall of gallbladder - likely benign. (C,D) Another case displaying large irregular polypoidal soft tissue thickening in gallbladder fundal region (white arrow) with cholelithiasis (black arrow) on USG; postcholecystectomy histopathological examination revealed adenocarcinoma")
 Photomicrograph [2X (A) and 40X(B); hematoxylin-eosin stain] shows the mucosa as a single layer of columnar epithelium with underlying lamina propria (thick arrows), irregular muscle layer (thin arrows), and connective tissue (arrowheads).")
 showing branching fibrovascular stalks lined by atypical cuboidal or columnar cells.")
 shows neoplastic epithelial cells with abundant intracytoplasmic mucin, which displaces the nuclei to the periphery (arrow).")
 shows nests of well-differentiated, neoplastic, keratinizing squamous cells (arrow) that infiltrate the gallbladder wall.")
 shows focal neoplastic mural thickening involving the body and neck region of gallbladder(arrow). Scale is in centimeters")
 Ultrasound images showing a large illmarginated heterogeneously hypo-echoic mass lesion replacing gallbladder (arrow) with adjacent hepatic infiltration (arrowhead). Note echogenic focus with distal acoustic shadowing within the mass lesion suggestive of calculi (black arrow).")
 Axial and coronal contrast enhanced CT images showing heterogeneously enhancing lobulated soft tissue mass lesion replacing gallbladder with adjacent hepatic (white arrow) and colonic (hepatic flexure) infiltration (black arrow). In addition, moderate ascites is also noted.")
In a known case of cholelithiasis, ultrasound images reveal: (A)distended gallbladder with multiple intraluminal calculi (black arrow)and layering of sludge, (B)annular mural thickening in neck region of gallbladder (white arrow) with, (C) periportal/peripancreatic and (D) pre/paraaortic lymphadenopathy.")
 Same patient underwent contrast enhanced CT and radical cholecystectomy with lymph node dissection: (A,B) Coronal and axial CT images reveal cholelithiasis (black arrow) with annular mural thickening in gallbladder neck region (white arrows) and periportal/peripancreatic, pre/para-aortic lymphadenopathy (yellow arrows) (C) Photograph of resected gallbladder (cut specimen) shows focal neoplastic mural thickening involving the body and neck region of gallbladder(arrowhead) (D) Photomicrograph(10X; HE stain) revealed well differentiated adenocarcinoma of gallbladder.")
 A 56 year old lady presented with pain abdomen; (A) Ultrasonography revealed cholelithiasis (black arrow) with polypoidal soft tissue thickening in gallbladder fundal region (white arrow), Subsequently MRI confirmed polypoidal mass in fundus of gallbladder displaying T2 hyperintensity on coronal T2WI (B). Later cholecystectomy was performed and histopathological examination revealed mucinous adenocarcinoma.")
 Case of advanced carcinoma of gallbladder; (A,B) Coronal T2WI and thick slab 2D MRCP images reveal large mass replacing gallbladder with surrounding hepatic infiltration (arrowhead) and extension to hilar region (white arrow) with resultant hilar block and attendant moderate upstream biliary dilatation. (C,D) DWI and axial T2WI reveal hepatic and pulmonary metastases(black arrows).")
 A case of locally advanced carcinoma of gallbladder; (A,B) Contrast enhanced axial CT and (C,D)coronal T2W MR images reveal diffuse asymmetric circumferential mural thickening of gallbladder (white arrows) with adjacent hepatic (arrowhead) and duodenal infiltration (white arrow) and contiguous extension along cystic duct to involve proximal third of common duct (black arrow) and resultant upstream biliary dilatation.")
 A case of carcinoma gallbladder; contrast enhanced (A) axial and (B) coronal sections of abdomen reveals, annular asymmetric mural thickening of gallbladder with adjacent hepatic infiltration (white arrow) and characteristic enlarged (>10mm), ring enhancing pancreatoduodenal, para-aortic and superior mesenteric lymphnodes (black arrows).")
 A case of carcinoma gallbladder; contrast enhanced axial sections of (A) abdomen and (B) chest reveals, annular asymmetric mural thickening of gallbladder with adjacent hepatic infiltration (white arrow) and hepatic and pulmonary metastases (black arrows).")
 with surrounding mesenteric fat stranding in subhepatic region and adjacent colonic infiltration (arrowhead) with moderate ascites and nodular enhancing peritoneal thickening (black arrows) in keeping with intraperitoneal spread of carcinoma gallbladder.")
 Axial and coronal reformatted contrast enhanced CT images; A case of advanced carcinoma gallbladder with hepatic infiltration (white arrows) and hilar block (black arrows) with PTBD sent (arrowheads) and pneumobilia (thin black arrows).")
 Staging References: Gallbladder carcinoma: radiologic-pathologic correlation. Radiographics. 2001 Mar-Apr;21(2):295-314; questionnaire, 549-55.")
:295-314; questionnaire, 549-55.")
:295-314; questionnaire, 549-55.")
 Axial and (B) Coronal T2W MR images reveal diffuse symmetric T2 hyperintense gallbladder wall thickening (white arrows) with T2 hypointense intraluminal calculi (black arrow) and mild pericholecystic fat stranding.")
 Axial contrast enhanced CT and (B) Axial post contrast T1W MR images reveal heterogeneously enhancing lobulated gallbladder wall thickening (white arrows) with poorly enhancing intramural areas (black arrows). (C) Coronal MR images reveal attendant biliary dilatation (small white arrows). (D) High power view showing dense inflammation comprising of foamy macrophages, lymphocytes, neutrophils & foreign body type of giant cells. References: Images reproduced from: Arora A, Puri SK, Upreti L, Kapoor A, Vandana. Xanthogranulomatous cholecystitis masquerading as gallbladder carcinoma, {Online}. DOI: 10.1594/EURORAD/CASE.8648")
 Axial contrast enhanced CT images reveal diffuse gallbladder wall thickening with intramural cystic spaces. Note is made of cirrhotic liver architecture with splenomegaly , multiple abdominal collaterals and portal vein thrombosis. (B) Photomicrograph (40X;HE stain) shows glands in the muscle layer with stroma- Adenomyomatous changes.")
.")
 Axial contrast enhanced CT and (C) coronal reformatted images reveal lobulated heterogeneously enhancing mass lesion involving left lobe of liver (arrows) in close proximity to gallbladder. Differentials include mass forming intrahepatic cholangiocarcinoma and carcinoma gallbladder with hepatic infiltration.")