ECR 2015 / C-1889
Detection of bone erosions in rheumatoid arthritis with cone beam computed tomography compared with magnetic resonance imaging
This poster is published under an open license. Please read the disclaimer for further details.
Congress:
ECR 2015
Poster Number:
C-1889
Type:
Scientific Exhibit
Keywords:
Musculoskeletal bone, Musculoskeletal joint, Cone beam CT, MR, Comparative studies, Cost-effectiveness, Arthritides
Authors:
E. Trajcevska, C. Owen, R. Buchanan, R. B. Zwar; Melbourne/AU
DOI:
10.1594/ecr2015/C-1889
.
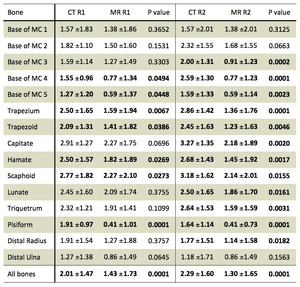
Clinically significant p values are highlighted by bold text.
R1: Reader 1. R2: Reader 2. MC: Metacarpal.")
Table 1:
Mean number of erosions per bone (mean ±standard deviation).
Clinically...

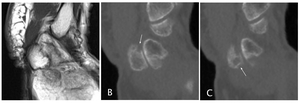
Fig. 5:
Pisiform: Sagittal imaging. A. PD MRI. B, C. CBCT. Comparison of imaging of the...
. A nutrient foramen of the scaphoid bone is better appreciated on CBCT (dotted arrow).")
Fig. 6:
Metacarpals; Scaphoid: Coronal imaging. A. Post Contrast Fat Sat T1 Weighted...
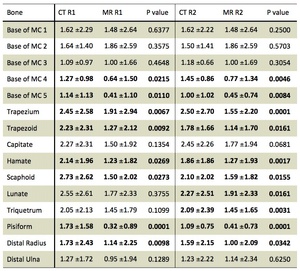
, based on the OMERACT-RAMRIS scoring system. Bone erosion was scored 1- 10, according to the proportion of bone involvement (in increments of 10%).
Clinically significant p values are highlighted by bold text.
R1: Reader 1. R2: Reader 2. MC: Metacarpal.")
Table 2:
Proportion of bone involvement scores (mean score per bone; mean ±standard...