ECR 2015 / C-1911

Cervical Thymic Anomalies: A Pictorial Review
This poster is published under an open license. Please read the disclaimer for further details.
Congress:
ECR 2015
Poster Number:
C-1911
Type:
Educational Exhibit
Keywords:
Congenital, Normal variants, eLearning, Ultrasound, MR, CT, Head and neck
Authors:
S. M. Tochetto, O. C. Saito, J. D. Zavariz, M. C. Chammas; São Paulo/BR
DOI:
10.1594/ecr2015/C-1911

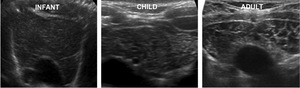
Fig. 3:
Ultrasonographic images of a normal thymus in an infant, a child and an adult.
. References: Department of Radiology, Clinics Hospital, University of São Paulo, SP, Brazil")
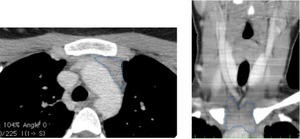
Fig. 4:
Axial and reconstructed coronal CT images show the normal appearance of thymus...

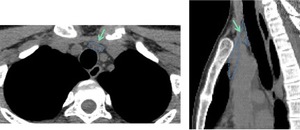
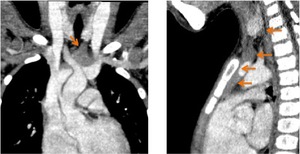
Fig. 5:
Axial and reconstructed sagittal CT images of a 12 years old girl referred to...
 of the cervical component of the thymus. References: Department of Radiology, Clinics Hospital, University of São Paulo, SP, Brazil")
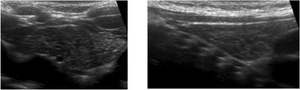
Fig. 6:
Corresponding axial and longitudinal US images of the same patient presented in...
. References: Department of Radiology, Clinics Hospital, University of São Paulo, SP, Brazil")
Fig. 7:
Longitudinal and axial US images of a 9 months old girl referred to our...
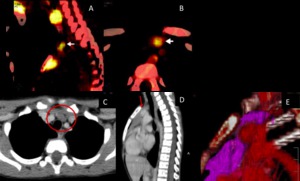
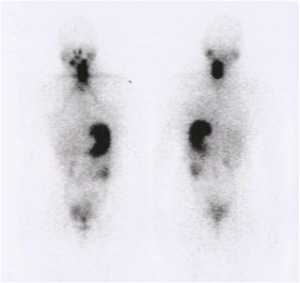
 and axial (B) PET-CT images of 28 years old man demonstrated a nodular FDG-uptake in the anterior lower neck in the midline region. Axial (C), sagittal (D) and tridimensional reconstructed (E) CT images after IV contrast demonstrated that the FDG-uptake corresponded to the superior extension of the thymus. References: Courtesy of Dr Miguel Francisco Neto, Dr.Cristiane Wosny, Dr. Regina Lucia E. Gomes e Dr. Rodrigo Gobbo Garcia)")
Fig. 8:
Sagittal (A) and axial (B) PET-CT images of 28 years old man demonstrated a...

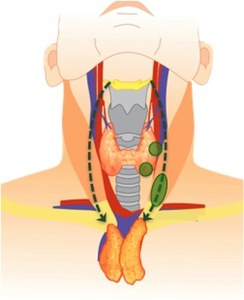
Fig. 9:
Ectopic cervical thymic tissue frequent sites.

Fig. 10:
15 years old female referred for evaluation of a cervical mass. Longitudinal US...
 and common carotid artery (CA) (dashed line). References: Department of Radiology, Clinics Hospital, University of São Paulo, SP, Brazil")
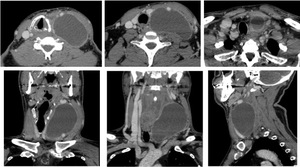
Fig. 11:
Coronal and axial CT images after IV contrast agent in a 15 years old female....
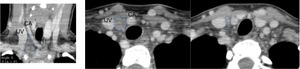
 Longitudinal and axial US images show a hypoechogenic and slightly heterogeneous nodule with multiple hyperechogenic foci situated adjacent to lower pole of the left thyroid lobe in a 11 years old boy. (C - F) Corresponding axial, coronal axial sagittal CT images after IV contrast agent show a nodular soft tissue image adjacent to lower pole of the left thyroid lobe.
References: Department of Radiology, Clinics Hospital, University of São Paulo, SP, Brazil")
Fig. 12:
(A and B) Longitudinal and axial US images show a hypoechogenic and slightly...
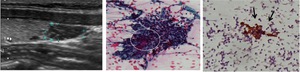
 numerous lymphocytes (thymocytes) and a large epithelial cell (circle). Cytokeratin immunostaining shows an epithelial cells intensely positive for cytokeratin, characteristic finding of the thymic epithelial cells (arrows). References: Department of Radiology, Clinics Hospital, University of São Paulo, SP, Brazil")
Fig. 13:
Photomicrography of the FNA cytology demonstrated (A) numerous lymphocytes...
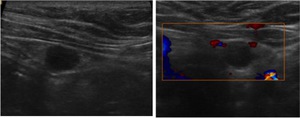
. The ectopic thymic tissue has poor vascularization on US Doppler image. References: department of Radiology, Clinics Hospital, University of São Paulo, SP, Brazil")
Fig. 14:
14 years old male. US images show ectopic thymic tissue in the left lower...

Fig. 15:
The sonographic evaluation of a 7 months old boy demonstrated:
-...

Fig. 16:
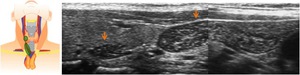
Longitudinal US images in a 5 years old girl. Ectopic thymic tissue is...

Fig. 17:
Longitudinal US images in a 12 years old girl. Ectopic thymic tissue is...
. References: Department of Radiology, Clinics Hospital, University of São Paulo, SP, Brazil")
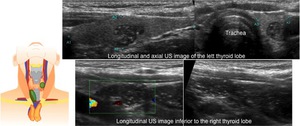
Fig. 18:
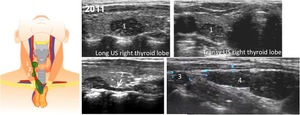
Ectopic thymic tissue is identified inside the right thyroid lobe and along the...
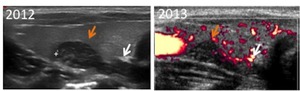
 and two years (2013) after the first evaluation (2011), do not demonstrate size or morphologic changes in the ectopic thymic tissue. References: Department of Radiology, Clinics Hospital, University of São Paulo, SP, Brazil")
Fig. 19:
Sonographic images of the same patient presented in Fig 18, performed one...

Fig. 20:
Reconstructed coronal and saggital CT imagines demonstrate ectopic thymic...
")
Fig. 21:
131I whole-body scanning revealed an abnormal 131I uptake in the left cervical...
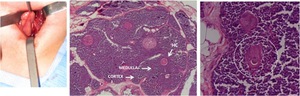
 and and the inner medulla (lighter staining region). The cortex stains more darkly than the medulla, because it contains more lymphocytes (thymocytes).
Hassall’s corpuscles (circle) are a characteristic feature of thymic medulla. These structures are only found in the thymus and are composed of a concentric arrangement of flattened thymic epithelial cells. The center of Hassall’s corpuscles is keratinized.
References: (Courtesy of Dr Marília D’Elboux Guimarães Brescia, Dr Adriano Ibrahim Asse Lopes)")
Fig. 22:
Photomicrographs of the surgical specimen demonstrated the two anatomically and...

Fig. 23:
US images of abnormal parathyroid glands

Fig. 24:
Hypoechoic thyroid nodule that was a papillary thyroid carcinoma

Fig. 25:
Cervical lymphadenomegaly

Fig. 26:
Lipoma

Fig. 27:
Longitudinal and axial US images show a anechoic unilocular cyst situated in...

Fig. 28:
The axial, coronal reconstructed and sagittal recontructed CT images after IV...

Fig. 29:
Branchial cleft cyst

Fig. 30:
Cystic hygroma