ECR 2015 / C-1933
Budd-Chiari: diagnosis, follow up after intervention and pitfalls - a pratical guide using Doppler ultrasound
This poster is published under an open license. Please read the disclaimer for further details.
Congress:
ECR 2015
Poster Number:
C-1933
Type:
Educational Exhibit
Keywords:
Obstruction / Occlusion, Grafts, Education and training, Stents, Diagnostic procedure, CT, Ultrasound-Colour Doppler, Ultrasound, Vascular, Liver, Abdomen
Authors:
J. D. Zavariz1, S. M. Tochetto2, F. L. Pereira1, T. N. Oliveira1, M. C. Chammas1; 1São Paulo/BR, 2Chicago, IL/US
DOI:
10.1594/ecr2015/C-1933

Fig. 1:
B-mode ultrasound. Longitudinal view of right liver's lobe, which presents...
, separated by the fissure of venous ligament. In this image a large (hypertrophied) segment I is seen. References: Instituto de Radiologia - Hospital das Clinicas da Faculdade de Medicina da Universidade de São Paulo - Brazil")
Fig. 2:
B-mode ultrasound. Longitudinal view of the lateral segment of the left lobe...

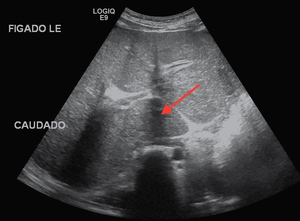
Fig. 3:
B-mode ultrasound - subcostal view. The red arrow points to a prominent segment...
 confluence of the three major hepatic veins into IVC. References: Instituto de Radiologia - Hospital das Clinicas da Faculdade de Medicina da Universidade de São Paulo - Brazil")
Fig. 4:
B-mode ultrasound. Oblique view of the upper part of the liver demonstrate the...
. Only the left vein is slighted depicted, with a reduced caliber. References: Instituto de Radiologia - Hospital das Clinicas da Faculdade de Medicina da Universidade de São Paulo - Brazil")
Fig. 5:
B-mode ultrasound . Subcostal view of the liver showing the section in which it...
, multi-phasic, homogenous flow is seen with patent veins in all extension (not demonstrated). References: Instituto de Radiologia - Hospital das Clinicas da Faculdade de Medicina da Universidade de São Paulo - Brazil")
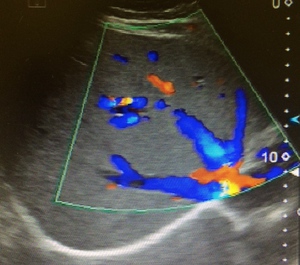
Fig. 6:
Color Doppler ultrasound. Normal confluence of the three major hepatic veins...
. Note that the velocity rate is set at an extremely low rate. References: Instituto de Radiologia - Hospital das Clinicas da Faculdade de Medicina da Universidade de São Paulo - Brazil")
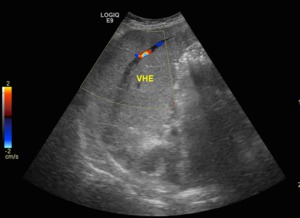
Fig. 7:
Color Doppler ultrasound. Longitudinal view of liver's left lobe. Hypoechogenic...
. Although the right hepatic vein is normal (red "R"), the left hepatic vein (red "L") has a small caliber and in the normal anatomic place of the middle hepatic vein (red "M) nothing is seen. References: Instituto de Radiologia - Hospital das Clinicas da Faculdade de Medicina da Universidade de São Paulo - Brazil")
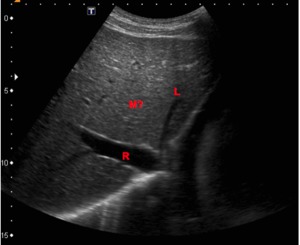
Fig. 8:
B-mode ultrasound (subcostal view of the liver). Although the right hepatic...
, a monophasic form is seen, resulting from thrombosis of two hepatic veins. References: Instituto de Radiologia - Hospital das Clinicas da Faculdade de Medicina da Universidade de São Paulo - Brazil")
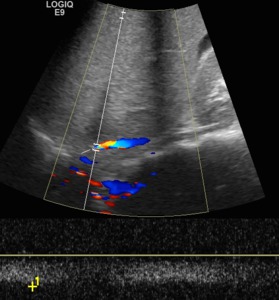
Fig. 9:
Triplex Doppler ultrasound. Right parasagital view - longitudinal inferior vena...

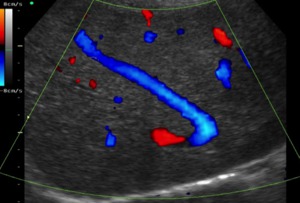
Fig. 10:
Color Doppler - longitudinal view of the segment I. The curvilinear shape are...

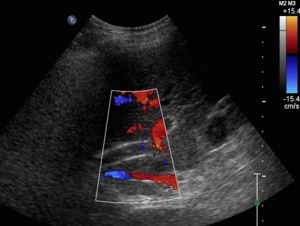
Fig. 11:
B-mode ultrasound. The collaterals in "comma" shape near the cava vein are seen...

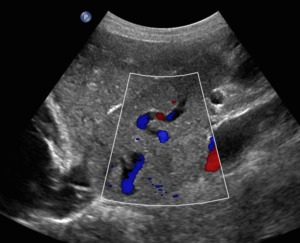
Fig. 12:
Color Doppler ultrasound. In the subcostal view a colateral mimicking the...

Fig. 13:
Color Doppler ultrasound. Despite the low velocity scale, absence of flow is...
. References: Instituto de Radiologia - Hospital das Clinicas da Faculdade de Medicina da Universidade de São Paulo - Brazil")
Fig. 14:
B-mode ultrasound. The extremity of the TIPS is at the right portal vein. Just...
. The measurement at this and in a previous point shows a velocity gradient of more than 100cm/s (not shown), in keeping with stenosis. References: Instituto de Radiologia - Hospital das Clinicas da Faculdade de Medicina da Universidade de São Paulo - Brazil")
Fig. 15:
Color Doppler ultrasound. The velocity range is set to analise the TIPS....