ECR 2015 / C-2047
Benign pathology of the salivary glands.
This poster is published under an open license. Please read the disclaimer for further details.
Congress:
ECR 2015
Poster Number:
C-2047
Type:
Educational Exhibit
Keywords:
Ear / Nose / Throat, Head and neck, Ultrasound, CT, MR, Education, Education and training, Pathology
Authors:
G. Price, S. R. Rice, S. Patel, S. Morley, T. Beale; London/UK
DOI:
10.1594/ecr2015/C-2047
. (2000). Practical head and neck ultrasound. Cambridge University Press.")
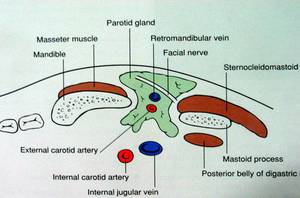
Fig. 1:
Anatomy of the parotid gland in axial section

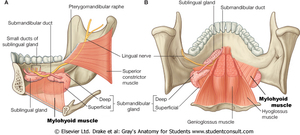
Fig. 2:
Anatomy of the submandibular and sublingual glands

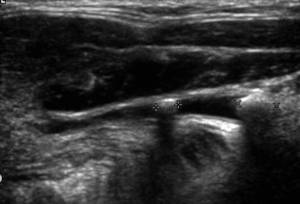
Fig. 3:
Ultrasound probe position for visualisation of the submandibular duct.

Fig. 4:
Parotid gland duct post and pre sialogogue

Fig. 5:
Ultrasound of the submandibular duct demonstrating two ductal calculi with...
")
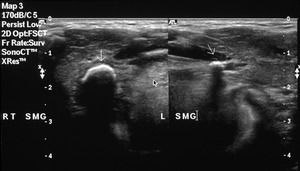
Fig. 6:
Ultrasound of both submandibular glands demonstrating bilateral calculi (arrows)

Fig. 7:
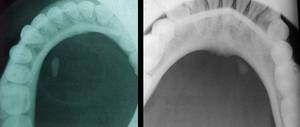
Plain occlusal radiographs demonstrating distal submandibular duct stones

Fig. 8:
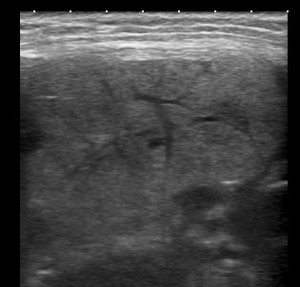
Ultrasound of the left submandibular gland demonstrating acute sialadenitis

Fig. 9:
Ultrasound parotid - Sjogren's syndrome

Fig. 10:
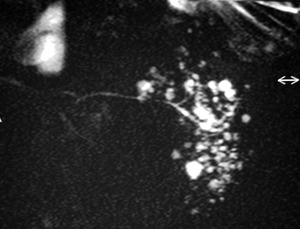
MR sialogram - Sjogrens syndrome

Fig. 11:
Ultrasound of the submandibular gland in a patient with HIV - note the large...

Fig. 12:
Ultrasound parotid - Pleomorphic adenoma
, pathology proven mucoepidermoid tumour.")
Fig. 13:
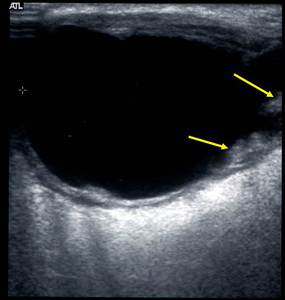
Cystic lesion within the parotid gland (see also MRI), pathology proven...
, pathology proven mucoepidermoid tumour.")
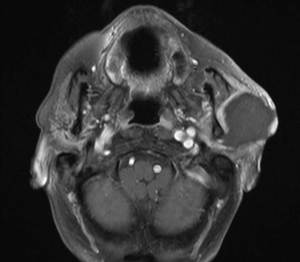
Fig. 14:
Cystic lesion of the left parotid gland (see also ultrasound image), pathology...