A) ENTITIES THAT PRIMARILY AFFECT TUNICA INTIMA
1.
MID-AORTIC SYNDROME
Rare aortic coarctation that occurs in children.
Frequently involves the renal arteries.
Its ethiopathogenesis is discussed.
Hystologically is due to distorsion and fibrosis of intimal and elastic internal lamina
Idiopathic type: good prognosis.
2ry type: associated with Takayasu arteritis and Williams syndrome.
ULTRASOUND:
- Parvus-tardus doppler waveform
- Diminished RI
ANGIOGRAPHY:
- Segmental abdominal aorta stenosis
- Renal artery stenosis
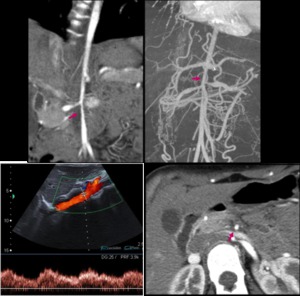
Fig. 2: 14yo girl with altered renal function underwent color doppler US, demonstrating a parvus-tardus waveform in abdominal aorta. CT angiography was performed to confirm segmental stenosis at the origin of renal arteries (arrows).
2.
PENETRATING ULCER
In patients with advanced atherosclerosis.
Most common in descending thoracic aorta.
Ethiopathogenesis: Deep ulcer in atherosclerotic plaque that penetrates intima inducing medial exposure to arterial flow.
This origins an hemorrhage that triggers an intramural hematoma.

Fig. 3: Intramural hematoma formation
Follow-up is needed because it may evolve to aortic dissection.
US: Protrusion of aortic lumen into thickened wall
CT:
- Focal pouching into the thickened wall without intimal flap.
- Adjacent focal aortic hematoma.
- Extensive atherosclerosis.
MR:
- Focal crater-like protrusion
- Mural hematoma: hyperintense on T1W during acute phase.

Fig. 4: Focal crater-like protection (pink arrow) into an eccentric intramural hematoma (yellow arrow) in a patient with severe chest pain compatible with penetrating ulcer.
3.
GIANT CELL ARTERITIS
Women,
>50 yo.
Typically affects aortic arch and branch vessels.
Ethiopathology:
- Myofibroblastic proliferation induces INTIMAL HYPERPLASIA that leads to OCCLUSIVE VASCULOPATHY
- Mononuclear infiltration,
granulomas and giant cells growth lead to wall weakening that may trigger ANEURYSMS (in end stage disease)
US: Hypoechogenic wall thickening.
The ‘halo sign’ translates active inflammation.
CT:
- Concentric hypodense intimal wall thickening
- Possible perivascular cuffing
MR:
Wall edema: hyperintense in T2W and STIR (meaning active inflammation)
Marked enhancement of the arterial wall
The degree of edema and enhancement correlates with the systemic inflammation.
FDG-PET: Uptake in active phase
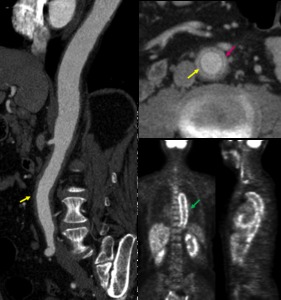
Fig. 5: Diffuse aortic wall thickening (yellow arrow) with perivascular cuffing (pink arrow) and intense uptake in FDG-PET meaning active aortitis in a 64yo woman with histologically confirmed giant cell arteritis.
4.
ATHEROSCLEROSIS
Chronic inflammatory response to colesterol exposure.
Most common in abdominal aorta.
Subendothelial accumulation of macrophages in vessel lumen -->
proliferation of smooth muscle cells --> lipid ingestion (foam cells)
--> ATHEROMA PLAQUE
Calcification between vessel wall and atheromatous plaques in older lesions.
US:
- Thickening of intima-media complex
- Turbulent flow in colordoppler
CT:
- Focal irregular thickening protruding into the lumen
- Calcification in outer border of the atheroma plaque
5.
FIBROMUSCULAR DYSPLASIA
Middle-aged women.
Non-inflammatory entity.
It is classified depending on which arterial layer is affected and the lesion composition.
INTIMAL FIBRODYSPLASIA:
<10% of all fibromuscular dysplasias.
Most common in children.
Collagen deposits around intima,
thickening the vessel wall.
ANGIOGRAPHY: Concentric and smooth narrowing
6.
INTIMAL ANGIOSARCOMA
Elderly men
Rare aortic malignant mesenchymal tumor.
Irregular soft-tissue mass protruding into the aortic lumen.
CT:
- Polipoid intraluminal soft tissue mass simulating an atheromatous plaque
- Poor enhancement.
MR:Tumoral enhancement
FDG-PET: Marked uptake
B) ENTITIES THAT PRIMARILY AFFECT TUNICA MEDIA:
1.
AORTIC COARCTATION
Most frequent congenitalaortic anomaly,
most common in males.
Narrowing of the aortic lumen due to an abnormal prominent posterior infolding of tunica media.
- Infantile: pre-ductal coarctation,affecting a long segment,
patent ductus arteriosus.
- Adult:juxta/post-ductal,
affecting a short segment.
Complications: heart failure,
dissection,
mycotic aneurysm.
Associated to bicuspid aortic valve,
ventricular septal defects,
cyanotic congenital diseases and mitral valve defects.
CT and MR ANGIOGRAPHY:
- Narrowing of aorta at distal arch or descending aorta
- Collateral circulation
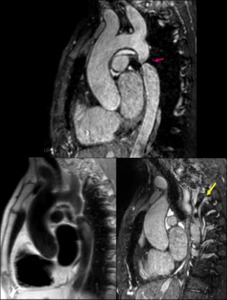
Fig. 6: Black-blood and White-blood sagital MR images showing focal aortic juxtaductal narrowing (pink arrow) with prominent colateral vessels (yellow arrow) in a 35yo male.
2.
MARFAN SYNDROME
Heritable connective tissue disorder. Young patients
Typically affects the aortic root.
It is also associated with bicuspid aortic valve.
Ethiopathology: Extensive loss and fragmentation of elastic fibers causing cystic medial degeneration that weakens the aortic wall and leads to vessel dilatation.
Complications: aortic dissection,
rupture.
CT:
- Dilatation of the aortic root
- Rare intimal calcification/thrombus.
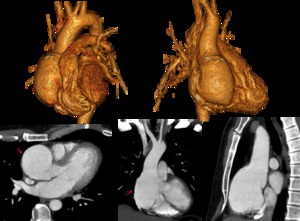
Fig. 7: Multiplanar contrast-enhanced CT and 3D VR images demonstrate dilatation of aortic root (pink arrow) associated with bicuspid valve in a young male with Marfan syndrome.
3.
INTRAMURAL HEMATOMA
It is an acute aortic syndrome (35%)
94% is HTA related,
6% post-traumatic.
May resolve or evolve toward aneurysm or dissection.
Ethiology: Hemorrhage of vasa vasorum within tunica media without intimal tear.
CT:
- ↑ aortic diameter
- Intimal curvilineal calcifications displaced inwards.
- Crescentic wall thickening
- Non contrast scan: Hyperattenuating
- Post contrast scan: Remains unenhanced
MR:
• Acute stage:
- T2 GRE (white blood): hyperintense
- T1 SE (black-blood): isointense
• Subacute/chronic stage:
- T2 GRE (white-blood): intermediate signal
- T1 SE (black-blood): hyperintense
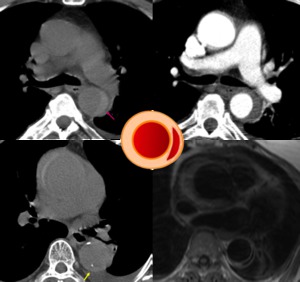
Fig. 8: Upper row: spontaneous hyperdense wall rim in descending aorta without posterior contrast enhancement.
Bottom row: NECT depicting displacement of intimal calcifications and axial T1 black-blood in a female with iodated-contrast allergy showing isointense crescentic thickening in ascending aorta and hypointense thickening in descending aorta (acute hematomas)
4.
AORTIC DISSECTION
Acute aortic syndrome.
Ethiology:
• Spontaneous: elderly HTA patients
• Intramural hematoma progression
• Penetrating ulcer progression
Tearing of intima and internal layer of media that allows blood entry within media forming a FLAP with double lumen.
CT and MRI:
- Medial displacement of intimal calcifications
- Intimal flap (classic or circunferential)
• TRUE LUMEN: Normal aortic lumen.
Early enhancement,
presence of beak sign: wedge-shaped flap around true lumen.
• FALSE LUMEN: Blood within aortic wall.
Delayed enhancement,
possible lumen thrombosis,
usually bigger diameter.
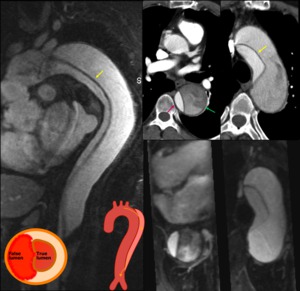
Fig. 9: Contrast-enhanced MR and CT in a 65yo female suffering from acute chest pain, clearly depicting an intimal flap (yellow arrow).
5.
BEHÇET DISEASE
Rare chronic inflammatory disorder most common in males.
Abdominal aorta is most frequently affected.
Destruction of media and fibrosis forming a saccular aneurysm.
Vasa vasoritis may lead to aneurysm or rupture.
CT:
- Lobulated eccentric pseudoaneurysms (possible thrombosed)
- Enhanced wall rim may be seen.
6.
SYSTEMIC LUPUS
Uncommon aortic involvement.
CT: Diffuse wall thickening
MR: T2W hyperintense thickened wall
FDG-PET: High metabolic rate.
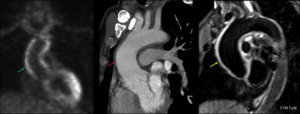
Fig. 10: FDG-PET, CT and MR showing diffuse ascending aorta thickening (pink arrow) with hyper signal in T2WI (yellow arrow) and increase FDG-uptake (green arrow) in suspected systemic lupus aortitis in a 50yo male.
7.
AORTIC ANEURYSMS
• Ascending aorta: frequently due to genetic disorders: Bycuspid aortic valve,
Ehler-Danlos syndrome,
Turner syndrome.
• Descending aorta: atherosclerosis related .
Saccular (eccentric) or fusiform (concentric).
Pathogenesis: Loss of medial muscle cells + macrophages infiltration leading to wall thinning and weakening,
that triggers focal vessel dilatation.
a) TRUE ANEURYSM: Contained by all layers.
US: Yin-yangsign in color doppler (bidirectional flow).
CT: Lumen dilatation ± mural thrombus or calcification.
b) FALSE / PSEUDOANEURISMS: Aortic wall breach,
only contained by adventitia.
May be traumatic or mycotic.
CT:
- Saccular multilobulated aneurysm.
- Adjacent soft tissue enhancement (inflammation)
- In mycotic aneurisms: possible lymphadenopathy and gas within the wall.
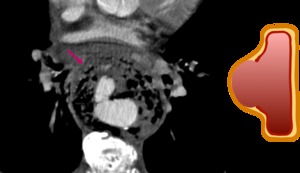
Fig. 11: Mycotic aneurysm with extensive gas formation and prominent periaortic inflammation.
8.
INFECTIOUS AORTITIS
a) BACTERIAL: Salmonella and Staphilococcus (bacteriemia)
b) SYPHILIS: Most frequent inascending aorta
First causes endarteritis that secondarily affects the elastic lamellae and causes collagen destruction by spirochetes,
that leads to dilatation and calcification.
Aneurysmal dilatation and aortic regurgitation.
c) TUBERCULOSIS: Usually from direct extension
Affecting distal aortic arch and descending aorta.
CT
- Thickening of aortic wall
- Aneurysmal dilatation: 90% Saccular aneurysm / pseudoaneurysm - Periaortic fluid or sof-tissue infiltration
- Air within aortic wall
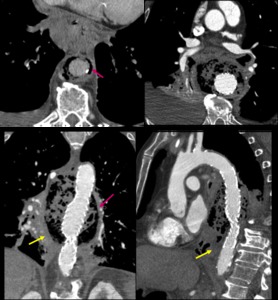
Fig. 12: Thoracic infectious aortitis with mediastinic inflammation after endoprotesis placement in a 82yo male with clinically suspected fistula and isolated Gram(+). Aortic wall gas (pink arrow) and periaortic infiltration (yellow arrow) are seen.
9.
FIBROMUSCULAR DYSPLASIA
a) MEDIAL FIBROPLASIA: 80%.
Alternating fibrotic areas and aneurysms.
Angiography: aspect of “beads on a string”
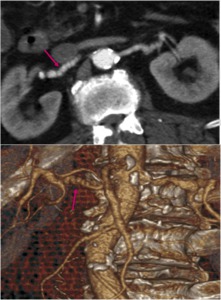
Fig. 13: Multiple focal stenosis in both renal arteries giving a string of beads appearance in a patient with medial fibroplasia.
b) PERIMEDIAL FIBROPLASIA: <10%.
Irregular wall thickening
Angiography: “Small beads on a string”.
c) MEDIAL HYPERPLASIA: 1-2%.
Excessive muscularproliferation.
Angiography: Smooth narrowing.
C) ENTITIES THAT PRIMARILY AFFECTS TUNICA ADVENTITIA
1.
TAKAYASU ARTERITIS
Chronic granulomatous disease.
Typically young women.
Usually affects aortic arch and its branches.
Segmental granulomatous infiltration:
• Early phase:adventitial infiltration + peri-vasavasorum cuffing
• Late: fibrosis and linear calcification (sparing ascending aorta)
CT:
- Wall thickening
- Poorly enhanced internal ring: swollen intima.
- Enhanced outer ring: inflamed media and adventitia.
MR:
• Acute phase:
- Thickened enhanced wall.
T2 hyperintense wall: mural edema
• Late phase:
- Descending aorta narrowing
- Ascending aorta dilatation.
- Abrupt vessel occlusion and collateral circulation
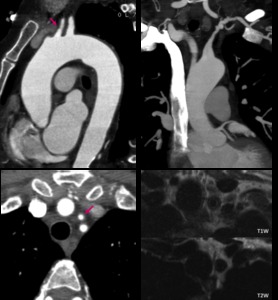
Fig. 14: Left carotid and left subclavian thickening (arrow) with stenotic areas from its origins; MR shows thickened wall with intermediate signal on T1W and low signal on T2W.
2.
PERIARTERIAL HYPERPLASIA
Rare type of fibromuscular dysplasia (1%).
Collagen extends into surrounding fat layers causing adventitial expansion with inflammation of aortic wall and surrounding area.
Fig. 15: Periarterial hyperplasia
3.
MURAL ANGIOSARCOMA
Extremely rare primary aortic sarcoma,
in elderly males.
Poor prognosis.
Exophytic growth invading periaortic structures.
Originates from adventitia or media and adventitia.
CT: Soft-tissue mass distorting the aortic wall with poor enhancement.
MR: Usually marked enhancement.
4.
INFLAMMATORY ANEURYSM:
Predominantly periadventitial involvement.
5% of aortic aneurysms,
most frequent in males.
Discussed ethiology.
Most common in abdominal aorta.
It is an aneurysm with marked aortic wall thickening of aortic and fibrosis extending to periaortic tissues.
US: Sonolucent halo around aorta
CT:
- Thickened aneurysmal dilatation.
- Perianeurysmal soft tissue cuffing with inflammatory signs,
sparing the posterior wall
- Enhancement after contrast administration.
MR: Perianeurysmal cuffing:
- Hypointense in T1W
- Hyperintense in T2W
- Enhancement after Gd administration
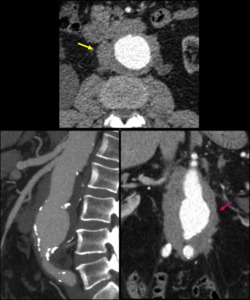
Fig. 16: Inflammatory aneurysm in a 45yo man with prominent periaortic soft-tissue infiltration sparing the prevertebral fat.
5.
RETROPERITONEAL FIBROSIS
• Idiopathic: discussed pathogenesis,
likely autoinmune (IgG related)
• 2ry: drugs,
radiotherapy,
infections,
trauma,
surgery.
- MALIGNANT: neoplastic,
poor prognosis
Typically involving the infrarenal aorta.
Ethiopathogenesis: Inflammatory and fibrotic periaortic tissue with proliferation of myofibroblasts and infiltration of lymphocytes,
plasma cells and macrophages.
CT:
- Irregular periaortic mass: isodense to the muscle.
• Malignant: more irregular
- No aortic displacement
- Marked enhancement in active phase that correlates with activity
- Frequent ureteral entrapment
MR:
- Periaortic soft tissue mass: Low signal on T1W
• Acute phase: Hyperintense on T2W with early contrast enhancement
• Chronic phase •Low signal on T2W with delayed enhancement
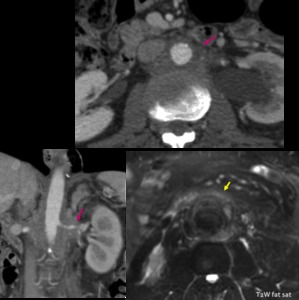
Fig. 18: Retroperitoneal fibrosis with irregular periaortic mass (pink arrow) and low signal on T2WI (yellow arrow) indicating chronic stage.
6.
ERDHEIM CHESTER DISEASE
It is a non-Langherhans histiocytosis of unknown ethiology.
1/3 affects the retroperitoneal space: soft tissue rim around kidneys Uncommon aortic involvement
Histologically is conformed of xanthogranulomatous infiltration and fibrosis.
CT:
- Concentric hypoattenuating periaortic soft tissue infiltration.
- Weak contrast enhancement
MRI
- Isointense to muscle signal on T1W and T2W
- Slight enhancement.
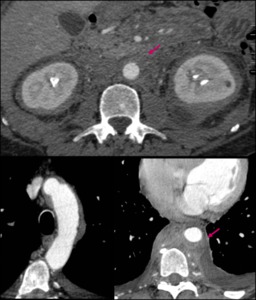
Fig. 17: Extensive soft-tissue proliferation around both kidneys and thoracic and abdominal aorta in a 41yo man with confirmed Erdheim-Chester disease.

.")

 into an eccentric intramural hematoma (yellow arrow) in a patient with severe chest pain compatible with penetrating ulcer.")
 associated with bicuspid valve in a young male with Marfan syndrome.")
")
.")
 with hyper signal in T2WI (yellow arrow) and increase FDG-uptake (green arrow) in suspected systemic lupus aortitis in a 50yo male.")

. Aortic wall gas (pink arrow) and periaortic infiltration (yellow arrow) are seen.")

 with stenotic areas from its origins; MR shows thickened wall with intermediate signal on T1W and low signal on T2W.")



 with prominent colateral vessels (yellow arrow) in a 35yo male.")
 and low signal on T2WI (yellow arrow) indicating chronic stage.")