The facial bones are bones surrounding the mouth and nose and contributing to the orbits; they include 14 bones: the paired maxillae,
zygomatic,
nasal,
lacrimal,
palatine,
and nasal conchae; and the unpaired vomer and mandible ( Fig. 1 ).
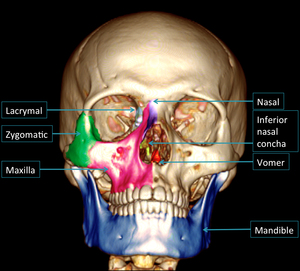
Fig. 1: Facial bones
References: Department of Radiology, La-Rabta Hospital, Tunis / Tunisia 2015.
The facial skeleton can be conceptualized as a series of buttresses: four transverse and four paired vertical buttresses ( Fig. 2 ).
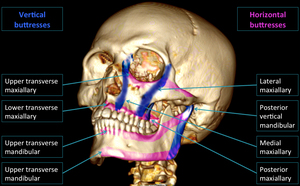
Fig. 2: Facial buttresses
References: Department of Radiology, La-Rabta Hospital, Tunis / Tunisia 2015.
The buttresses represent areas of relative increased bone thickness that support both the functional units and the form of the face in an optimal relation,
and interface with the skull base or cranium as a stable reference.
Disruption of the facial buttresses can alter normal function and change facial dimensions,
necessitating surgical fixation for restoration.
In order to plan exposure of the facial buttresses and restore them accurately,
the surgeon must have a thorough preoperative understanding of the degree and nature of their damage.
High-resolution multidetector computed tomography (CT) often provides the detail necessary for preoperative assessment of facial injuries.
It is crucial to expose the results by 2D multiplanar reformations in bone and soft tissue windowing and 3D volume rendering (VR).
Indeed the surgeon doesn’t operate on a report without imaging.
Also,
in complex maxillofacial fractures,
it is important to distinguish those that have direct surgical relevance.
To highlight the key imaging features that are critical for therapeutic management of the most common maxillofacial fractures,
we developed a checklist to be verified for each fracture group.
Nasal bone fractures ( Fig. 3 ):
Regarding fractures of the nasal bones,
the report must indicate if there is a comminution or displacement and associated fracture or hematoma of the nasal septum [2,
3].
This is to prevent nasal obstructive symptoms.
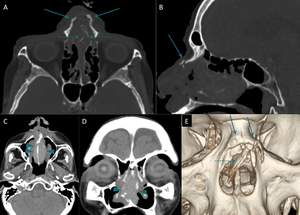
Fig. 3: Nasal fractures:
(A) Axial and (B) Sagittal CT reformations in bone windowing. (C) Axial and (D) coronal CT reformation in soft tissue windowing. (E) 3D VR reconstruction.
Bilateral comminuted fracture of the nasal bones (arrows). There is an associated fracture (small dotted arrows) and hematoma of the nasal septum (arrowheads).
References: Department of Radiology, La-Rabta Hospital, Tunis / Tunisia 2015.
Complex Naso-Ethmoïdo-Maxillo-Fronto-Orbital fracture (CNEMFO) ( Fig. 4 ):
For the complex naso-ethmoïdo-maxillo-fronto-orbital fracture,
it must be mentioned comminution of the medial orbital rim,
coronal distance between the two lacrimal fossae,
lacrimal duct injury,
nasofrontal duct disruption,
fracture of the posterior table of frontal sinus and/or the cribriform plate,
and associated intracranial abnormalities including pneumocephalus.
This is to prevent respectively avulsion of the medial canthus,
diplopia,
dacryocystitis,
frontal mucocele,
CSF leakage and anosmia [4,
5].
CNEMFO fracture may be incomplete and concerns only the maxillo-orbito-ethmoidal or naso-orbito-ethmoidal (NOE) complex.
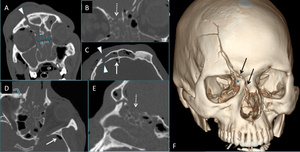
Fig. 4: CNEMFO fracture:
(A, B) Coronal, (C, D) axial and (E) sagittal CT reformations in bone windowing. (F) 3D VR reconstruction.
Central complex midface fracture combining: Factures of posterior and anterior tables of the right frontal sinus (arrowheads) with disjunction between the frontal process of the maxilla, the nasal process of the frontal and right nasal bone (black arrows). The medial orbital rim is not comminuted (star) and the distance between the two lacrimal fossae (A) is 28 mm (normal < 35mm). Injury of the nasolacrimal and nasofrontal ducts without disruption (curved arrow). Loss of substance of the cribriform plate (small dotted arrows). Pneumocephalus (white arrow).
References: Department of Radiology, La-Rabta Hospital, Tunis / Tunisia 2015.
Orbital fractures ( Fig. 5 ):
In orbital fractures,
it is necessary to look for integrity of the eyeball,
muscle and/or fat incarceration,
eno- or exophthalmos,
damage in the infra-orbital nerve,
intra-orbital bone fragments or conflicting on neurovascular structures and oculomotor muscles and intraorbital hematoma [6,
7].
Some of these lesions may indicate an urgent surgical treatment because the visual prognosis is at stake.
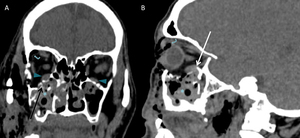
Fig. 5: Orbital floor fracture:
(A) Coronal and (B) Sagittal CT reformations in soft tissue windowing.
Comminuted fracture of the orbital floor with plugging of the lower rectus muscle by a bone splinter (white arrow). This muscle is enlarged compared to the contralateral side (arrowheads). The infra orbital nerve canal is damaged (black arrow).
There are also indirect signs of floor fracture: hemosinus right maxillary (star) and orbital emphysema (curved arrow).
References: Department of Radiology, La-Rabta Hospital, Tunis / Tunisia 2015.
Zygomatic fractures ( Fig. 6 ):
In zygomatic fractures,
the integrity of the orbital contents should always be sought and the degree of comminution or angulation can indicate surgical exposure [3,
8].
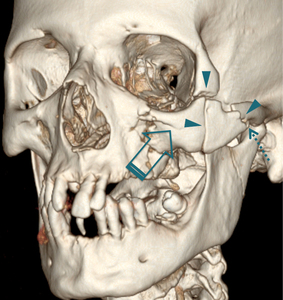
Fig. 6: Disjunction fracture of the zygomatic bone:
CT 3D VR reconstruction shows zygomatic disjunction fracture (arrowheads) with comminution of the zygomatic arch (dotted arrow) and impaction (solid arrow) of the zygoma.
We also note in this reconstruction a fracture of the orbital floor, a fracture of the anterior wall of the maxillary sinus through the infra orbital nerve canal and a low sub-condylar mandible fracture.
References: Department of Radiology, La-Rabta Hospital, Tunis / Tunisia 2015.
Le-Fort fractures [7,
9]:
Le-Fort fractures involve disruption of the pterygoid plates from the posterior maxilla.
Once a pterygo-maxillary disjunction has been diagnosed,
the remaining facial buttresses are inspected to determine the class of Le Fort fracture ( Fig. 7 ),
with possible combination of Le Fort I,
II,
and III.
We must seek in their context an associated fracture of the hard palate compounding the functional prognosis.
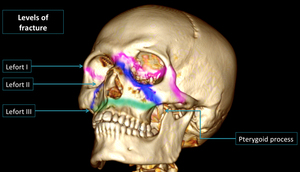
Fig. 7: Le Fort fractures:
CT 3D VR reconstruction shows the common Le Fort fracture patterns:
The Le Fort I pattern involves fractures through the inferior portions of the medial and lateral maxillary buttresses.
The Le Fort II pattern involves fractures through the zygomatico-maxillary and fronto-maxillary sutures.
The Le Fort III pattern involves complete craniofacial dissociation.
References: Department of Radiology, La-Rabta Hospital, Tunis / Tunisia 2015.
Fig. 8 shows an example of bilateral Le Fort fracture.
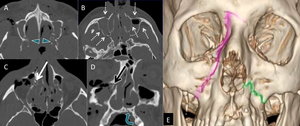
Fig. 8: Bilateral Le Fort fracture:
(A,B,C) Axial and (D) frontal CT reformations in bone windowing. (E) 3D VR reconstruction.
Transverse fracture of the face (Lefort II at right, Lefort I at left) associating: Fracture of the two pterygoid processes (arrowheads) and the maxillary walls (dotted arrow). Floor fracture of the right orbit (black arrow). Involvement of the right nasolacrimal duct (white arrow) and associated fracture of the left hard palate (curved arrow).
References: Department of Radiology, La-Rabta Hospital, Tunis / Tunisia 2015.
Mandibular fractures [5,
10]:
For mandibular fractures,
one must know the articular or extra-articular fractures,
displacement,
bilateralism and the passage through the toothed portion and/or the inferior alveolar nerve canal.
These findings guide to a functional or surgical treatment and whether antibiotherapy is necessary.
Fig. 9 illustrates the anatomy and the main lines of mandibular fracture.
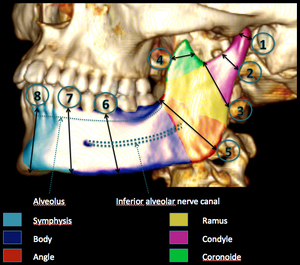
Fig. 9: Mandibular anatomy and fractures:
CT 3D VR reconstruction illustrating the anatomy and the main fracture lines on the left hemi-mandibule:
1: Coronoide fracture; 2: condylar fracture; 3: high subcondylar fracture; 4 low sub condylar fracture; 5: angular fracture; 6: fracture of the corpus passing through the root of the tooth 36; 7: parasymphysis fracture; 8: symphysis fracture.
References: Department of Radiology, La-Rabta Hospital, Tunis / Tunisia 2015.
Fig. 10 shows an example of bilateral complex mandibular fracture.
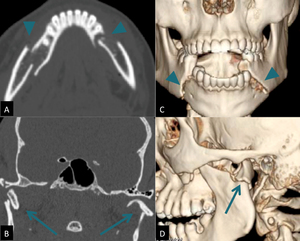
Fig. 10: Mandibular complex fracture:
(A) Axial and (B) frontal CT reformations in bone windowing and (C, D) 3D VR reconstructions.
Bilateral fracture of the corpus passing through the root of the teeth and through the inferior alveolar nerve canal (arrowheads) associated to bilateral low sub-condylar fracture with dislocation of the temporo-mandibular articulations (arrows).
References: Department of Radiology, La-Rabta Hospital, Tunis / Tunisia 2015.



 Axial and (B) Sagittal CT reformations in bone windowing. (C) Axial and (D) coronal CT reformation in soft tissue windowing. (E) 3D VR reconstruction.
Bilateral comminuted fracture of the nasal bones (arrows). There is an associated fracture (small dotted arrows) and hematoma of the nasal septum (arrowheads). References: Department of Radiology, La-Rabta Hospital, Tunis / Tunisia 2015.")
 Coronal, (C, D) axial and (E) sagittal CT reformations in bone windowing. (F) 3D VR reconstruction.
Central complex midface fracture combining: Factures of posterior and anterior tables of the right frontal sinus (arrowheads) with disjunction between the frontal process of the maxilla, the nasal process of the frontal and right nasal bone (black arrows). The medial orbital rim is not comminuted (star) and the distance between the two lacrimal fossae (A) is 28 mm (normal < 35mm). Injury of the nasolacrimal and nasofrontal ducts without disruption (curved arrow). Loss of substance of the cribriform plate (small dotted arrows). Pneumocephalus (white arrow). References: Department of Radiology, La-Rabta Hospital, Tunis / Tunisia 2015.")
 Coronal and (B) Sagittal CT reformations in soft tissue windowing.
Comminuted fracture of the orbital floor with plugging of the lower rectus muscle by a bone splinter (white arrow). This muscle is enlarged compared to the contralateral side (arrowheads). The infra orbital nerve canal is damaged (black arrow).
There are also indirect signs of floor fracture: hemosinus right maxillary (star) and orbital emphysema (curved arrow). References: Department of Radiology, La-Rabta Hospital, Tunis / Tunisia 2015.")
 with comminution of the zygomatic arch (dotted arrow) and impaction (solid arrow) of the zygoma.
We also note in this reconstruction a fracture of the orbital floor, a fracture of the anterior wall of the maxillary sinus through the infra orbital nerve canal and a low sub-condylar mandible fracture. References: Department of Radiology, La-Rabta Hospital, Tunis / Tunisia 2015.")

 Axial and (D) frontal CT reformations in bone windowing. (E) 3D VR reconstruction.
Transverse fracture of the face (Lefort II at right, Lefort I at left) associating: Fracture of the two pterygoid processes (arrowheads) and the maxillary walls (dotted arrow). Floor fracture of the right orbit (black arrow). Involvement of the right nasolacrimal duct (white arrow) and associated fracture of the left hard palate (curved arrow). References: Department of Radiology, La-Rabta Hospital, Tunis / Tunisia 2015.")

 Axial and (B) frontal CT reformations in bone windowing and (C, D) 3D VR reconstructions.
Bilateral fracture of the corpus passing through the root of the teeth and through the inferior alveolar nerve canal (arrowheads) associated to bilateral low sub-condylar fracture with dislocation of the temporo-mandibular articulations (arrows). References: Department of Radiology, La-Rabta Hospital, Tunis / Tunisia 2015.")