Main entities included in anomalous pulmonary venous connections are partial anomalous pulmonary venous connection(PAPVR),sinus venosus defect,
total anomalous pulmonary venousconnection(TAPVR),
cor triatriatum,
and pulmonary vein stenosis.
· Partial anomalous pulmonary venous connection (PAPVC)
Imaging Indications and Algorithm
The suggestion of anomalous venous return on chest radiography or echocardiography warrants further evaluation with cardiac CT angiography (CTA) or MRI.
Because of the increased frequency of PAPVC reported in patients with Turner syndrome,
routine screening in this population may be warranted.
[1]
Imaging Techniques and Findings
Radiography
Signs of right ventricular overload: a lateralized or upturned cardiac apex on the frontal radiograph and filling in of the retrosternal clear space on the lateral view.
Other findings: a dilated main pulmonary artery and increased pulmonary arterial vascular markings.
However,
chest radiography findings may be grossly normal.
Increased pulmonary blood flow is often present,
but it is nonspecific.
The abnormal vein itself may be visualized,
as in anomalous pulmonary venous drainage of the right lung to the IVC,
when the so-called scimitar vein (named for the crescent shape of the vessel likened to a Turko-Mongol saber) can be visualized,
also called the "scimitar sign." This sign is a linear opacity,
usually (but not always) found at the base of the right lung,
that widens as it courses inferiorly and ends in the inferior vena cava.
Vein gets larger as it descends towards the diaphragm.
It is associated with dextroposition of the heart due to right lung hypoplasia.
Hypoplasia may be mild or marked.
The scimitar sign can be obscured by a significant dextropositioning of the heart.
On the left lung we can observe: hyperinflation with large left pulmonary artery (depends on degree of hypoplasia right pulmonary artery).
Aberrant drainage into the SVC or azygos vein may result in dilation of these structures that is radiographically apparent.
Anomalous left pulmonary veins emptying into the left innominate vein can create a bulbous appearance of the superior mediastinum .
Rarely,
the increased flow volume may also be sufficient to dilate the superior vena cava (SVC),
widening the upper right mediastinal shadow.
This can simulate the so-called "snowman" heart shape described in total anomalous pulmonary venous return to a left vertical vein.
Ultrasonography
Echocardiography is often the first imaging modality employed to evaluate a child with suspected structural heart disease.
PAPVC has been diagnosed in utero. Defining the pulmonary venous connections is an integral step in every echocardiographic examination.
The pulmonary venous connections are often best demonstrated through a subxiphoid approach in infants.
Suprasternal,
parasternal,
apical,
and subcostal windows are often more revealing in older children.
When not all of the pulmonary venous connections can be accounted for,
a more detailed search for systemic connections is required.
The presence of dilated systemic veins can be a clue to an unsuspected anomalous venous connection.
The size or the diameter of the pulmonary veins should be determined by 2-dimensional (2D) echocardiography.
Spectral Doppler study of the individual pulmonary veins is also important to determine obstruction to the flow.
Right ventricular volume overload resulting from PAPVC is well evaluated with echocardiography.
Because of limitations in field of view of the pulmonary veins and left atrium from a transthoracic technique,
transesophageal scanning may be needed for more detailed anatomic study of the pulmonary vein insertion,
especially in the adult population.
[1]
In adults,
contrast echocardiography can help with the diagnosis.
Agitated saline in a left arm vein can reveal a negative contrast in the innominate vein at the side of the anomalous venous drainage from a left pulmonary vein.
In most patients,
transthoracic echocardiography can be performed to diagnose PAPVC and obviate the need for cardiac catheterization.
A high index of suspicion for the presence of the lesion is helpful to properly diagnose the condition.
Right ventricular dilation may be the first observation that indicates the presence of abnormal venous drainage.
The sonographer must identify all 4 pulmonary veins and visualize their connections to the heart.
The atrial septum also needs to be evaluated for defects.
[18]
Computed Tomography
CTA timed to maximize left atrial and pulmonary venous opacification provides high spatial resolution images of the course and connections of anomalous pulmonary veins.
The isotropic acquisition of current multidetector CT scanners allows multiplanar reformation,
maximum intensity projection,
and volume rendered reconstruction.
These techniques provide a degree of anatomic visualization previously available only with angiography.
In addition,
surrounding noncardiac structures,
such as the lung parenchyma,
are well demonstrated.
This can aid in the characterization of an associated hypoplastic or horseshoe lung.
Contrast-enhanced CT scanning is an alternative imaging modality to detect PAPVC when transthoracic images are limited,
especially in older children and adults.
Multislice CT scanning is useful in preoperative planning.
[1]
CECT (contrast-enhanced computed tomography)
1. Bronchial anomalies,
associated
• Absent minor fissure,
mirror imaging branching,
bilobed right lung
• Horseshoe lung: Bridge of lung fusing the two lungs across the posterior mediastinum
• Horseshoe lung: Ominous finding often associated with lethal cardiac anomalies
• Bronchial diverticula
2. Cardiovascular anomalies,
associated
• Dilated right ventricle in left-to-right shunts and pulmonary hypertension
• Enlarged main pulmonary artery
3. Anomalous vein
• Precisely define drainage into systemic vein
4. Occasional systemic arterialization of the lung from the descending thoracic aorta or upper abdominal aorta
HRCT
Hypoplastic lung: Mosaic perfusion with hypoattenuation of the hypoplastic lung.
Secondary bronchiectasis from recurrent infections.
Infections may be secondary to seeding of lung from bronchial diverticula.
[12]
Magnetic Resonance
Cardiac MRI is another useful tool for the evaluation of PAPVC.
MRI has been shown to be accurate in the evaluation of pulmonary vein anomalies and is often considered the method of choice for preoperative characterization of PAPVC.
Black blood images,
like CTA,
provide high spatial resolution for the evaluation of anatomic connections.
Phase contrast cine images allow accurate quantification of pulmonary and systemic blood flow for shunt fraction calculation.
Whereas the evaluation of lung parenchyma is less optimal than with CT,
the lack of ionizing radiation and the functional information about the quantification of right ventricular volume overload and shunt fraction make MR superior for guiding clinical management.
MRI is rapidly becoming the procedure of choice for further investigation of PAPVC. Although echocardiography findings suggest the PAPVC,
all the pulmonary veins may not be identified,
especially in adults.
With refinements in technology rapidly improving the quality of images obtained,
fewer children require invasive angiography.
Cardiac catheterization may be a more preferable diagnostic tool in infants with complex congenital heart conditions in whom PAPVC is one component.
Although echocardiography findings suggest the PAPVC,
all the pulmonary veins may not be identified,
especially in adults.
With refinements in technology rapidly improving the quality of images obtained,
fewer children require invasive angiography.
Cardiac catheterization may be a more preferable diagnostic tool in infants with complex congenital heart conditions in whom PAPVC is one component.
Use of MRI in the imaging of PAPVC revealed a characteristic sign termed the "broken ring sign." In individuals with normal anatomy,
a transverse MRI demonstrates a ringlike structure derived from mediastinal fat that surrounds the SVC.
In healthy individuals,
this ring is broken only at the point of entry of the azygous vein into the SVC.
In some patients with partial anomalous pulmonary venous return,
the ring of fat also appears to be breached or broken at the site of entry of the anomalous vein.
[1]
The advantages are that:
• is nonionizing
• better for cardiac shunts
The disadvantages are
· less useful for lung or bronchial anatomy
Classic Signs
The “scimitar” sign is a characteristic finding in right PAPVC.
The “snowman” sign,
although occasionally present in anomalous drainage of the left lung to the innominate vein,
is less prominent and less often appreciated in partial than in supracardiac total anomalous pulmonary venous connection.
· Total anomalous pulmonary venousconnection(TAPVR)
Imaging Indications and Algorithm
Nonspecific clinical findings: cyanosis or heart failure often lead to initial evaluation with chest radiography.
Echocardiography is also commonly performed early in the setting of unexplained cardiopulmonary disease.
Two-dimensional echocardiography with Doppler examination is often diagnostic; however,
when not all of the pulmonary venous drainage can be accounted for because of limitations in echocardiographic windows,
the next step should be cardiac MRI or CTA.
Imaging Techniques and Findings
Radiography
When the pulmonary venous connection to the systemic circulation is unobstructed,
cardiomegaly with right atrial and ventricular enlargement and increased pulmonary blood flow are present on the chest radiograph.
Patients with total drainage to the left innominate vein may demonstrate the „snowman sign”,
in which the upper portion of the snowman is derived from the vertical vein on the left,
the enlarged innominate vein superiorly,
and the enlarged SVC on the right.
The cardiac silhouette constitutes the lower portion of the snowman.
The chest radiograph appearance in patients with infradiaphragmatic
obstructed TAPVC is very different.
The heart size is normal or mildly enlarged,
and there is normal pulmonary blood flow with a variable degree of pulmonary edema,
depending on the degree of obstruction.
Ultrasonography
The lack of pulmonary veins entering the left atrium together with signs of right ventricular volume overload establishes the diagnosis of TAPVC on echocardiography.
At this point,
a detailed survey must be performed to account for all of the anomalous veins.
The individual veins should be carefully examined with two-dimensional and color Doppler techniques.
The size of the pulmonary veins at initial diagnosis has prognostic implications.
The orientation of aberrant vessels as well as presence or absence of obstruction should be clearly defined to aid surgical management.
Because of the association with heterotaxy syndrome,
the cardiac segmental anatomy and abdominal visceral morphology as well as intracardiac anomalies are also evaluated.
Computed Tomography
There are limited published data concerning the use of CTA for the evaluation of TAPVC.
The small studies that have been performed indicate that the modality is capable of demonstrating the anatomy of the pulmonary veins in detail.
[1] The course and size of the pulmonary veins can be determined with CTA,
and the presence of venous obstruction is well demonstrated with isotropic multidetector- row CT acquisition with multiplanar reformats,
maximum intensity projections,
and volume rendered techniques.
Functional assessment (particularly in the neonatal period) is well evaluated by echocardiography.
The pulmonary and abdominal visceral morphology is well demonstrated with CT,
aiding in the evaluation of patients with concomitant heterotaxy.
Magnetic Resonance
In patients with TAPVC who have incomplete evaluation of all of the anomalous pulmonary venous connections by echocardiography,
MRA can provide highly detailed comprehensive information.
The number of pulmonary veins and their sizes,
courses,
and drainage patterns are well depicted.Tthe size of the pulmonary veins is clinically relevant in that those patients with smaller and obstructed anomalous veins tend to have a worse outcome.[17]
Improved MRA techniques now allow excellent spatial resolution to detect the presence or absence of venous obstruction.
The anomalously draining veins should be carefully assessed for any intrinsic narrowing or extrinsic compression (i.e.,
from an adjacent pulmonary artery or bronchus).
Functional evaluation by MRI is often unnecessary in the neonate and is usually performed by echocardiography.
The cardiac segmental anatomy,
intracardiac and great vessel connections,
and abdominal visceral morphology in patients with heterotaxy can also be evaluated on MRI.
Classic Signs
The snowman sign or figure-eight appearance on chest radiography is the classic appearance of supracardiac TAPVC.
This appearance may be difficult to appreciate on a radiograph of an infant,
but it is more easily seen in older children with unrepaired TAPVC because of the progressive enlargement of the vessels carrying the anomalous pulmonary venous flow back to the right side of the heart.
· Sinus venosus defect
Imaging Indications and Algorithm
As described with PAPVC,
plain films and echocardiography are the initial and often the only necessary studies in the evaluation of SVD.
If the diagnosis is still uncertain,
cardiac MRI or CTA should be employed.
Imaging Techniques and Findings
Radiography
Plain film findings in SVD are nonspecific and include cardiomegaly with right-sided heart enlargement and increased pulmonary blood flow.
Ultrasonography
Echocardiography demonstrates abnormal continuity between the right upper lobe pulmonary vein and the SVC in the superior type of SVD.
Right atrial and ventricular enlargement is present,
and the atrial septumproper is intact.
Computed Tomography
Although there have been case reports,
no large case series has been published on the accuracy of CT in the evaluation of SVDs.The high spatial detail of CTA allows definition of the anomalous drainage.
Magnetic Resonance
Cardiac MR has been shown to be well suited for the evaluation of SVD.[1] In addition to defining the defect,
right ventricular volume and function and pulmonary- to-systemic blood flow ratio (shunt fraction) can be quantified.
MR angiography (MRA) can also depict additional pulmonary veins that may be connecting anomalously to the SVC or other systemic veins.
· Cor triatriatum
Imaging Indications and Algorithm
Imaging indications are the same as those described in the previous sections.
Imaging Technique and Findings
Radiography
In addition to otherwise unexplained pulmonary edema,
pulmonary artery enlargement may be seen secondary to pulmonary hypertension.
The heart is often small; however,
enlargement of the left atrium due to a dilated accessory chamber may be visualized.
Ultrasonography
Echocardiography is often the only modality needed in the evaluation of cor triatriatum.
Visualization of the thin echogenic membrane is often best appreciated through a parasternal,
apical,
or subcostal approach.
Supravalvular mitral stenosis due to a supramitral ring has an appearance similar to cor triatriatum and also results in venous obstruction.
The two entities can be differentiated by the location and appearance of the membrane.
The left atrial appendage and foramen ovale are located distal to the relatively thin curvilinear membrane of cor triatriatum, whereas the appendage and foramen are proximal to the stiff membrane of the supramitral ring.
Right atrial dilation and ventricular dilation secondary to venous obstruction are nonspecific and are seen in both diseases.
Computed Tomography
CTA can demonstrate the accessory chamber [1] and,
depending on the size of the membranous ostia,
may allow differentiation of drainage to the left or right atrium.
If the cor triatriatum is associated with partial anomalous venous connection,
these aberrant pathways can be well demonstrated.
As stated before,
the requisite ionizingradiation and the relative lack of functional informationpertaining to right-sided heart overload are drawbackscompared with MRI.
Magnetic Resonance
Like CTA,
cardiac MRI allows excellent anatomic depiction of the accessory atrial chamber in cor triatriatum.
Functional information about right-sided heart strain or overload may also be obtained.
Flow from the high-pressure accessory chamber through the obstructed membrane into the low-pressure left atrium can produce visible turbulent jets or dephasing on cine images.
Additional anomalies,
such as PAPVC and the presence of an ASD,
can be evaluated.[1]
Images for this section
Case 1: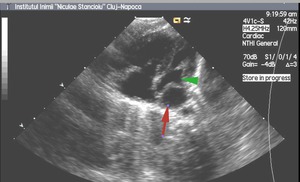
Fig. 4
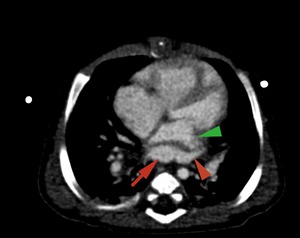
Fig. 5
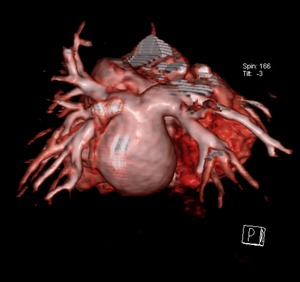
Fig. 6

Fig. 7
Fig.
4-7.
2 months old child with ASD,
coronary sinus type,
with TAPVR -all pulmonary veins (red arrowhead) drain into a common collector (red arrow) and then in the coronary venous sinus.The left atrium (green arrowhead) is located anterior of the pulmonary venous collector and is compressed; (4).echocardiography,
(5).
MDCT angiography - axial section ,
(6,7).
3D VRT reconstruction.
Emergency County Hospital, Radiology Department,
Cluj-Napoca/RO.
Case 2:

Fig. 8
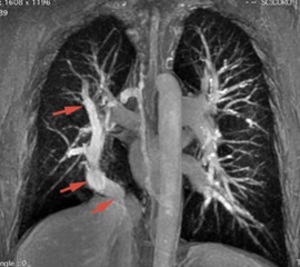
Fig. 9

Fig. 10
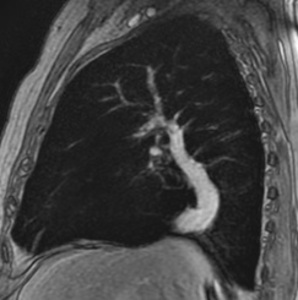
Fig. 11
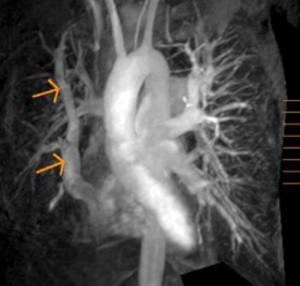
Fig. 12
Fig.
8-12. 51 years old patient,
with severe mitral stenosis,
echocardiographic diagnosed.
During preoperative catheterization were detected increased levels of oxygen in the IVC.
Chest radiography (8) –linear opacity with vascular appearance,
perihilar and infrahilar on the right,
with craniocaudal path – « Scimitar sign ».
MRI angiography was indicated; it showed PAPVR,
with right pulmonary venous blood drainage in a venous collector (arrows) that flows into the VCI - Scimitar syndrome.
(8) Axialsection SE T1; (9) Coronal angiography - MIP reconstruction; (10) Sagittal MRI angiography;(11) and (12) 3D MIP reconstruction.
Emergency County Hospital, Radiology Department,
Cluj-Napoca/RO.
Case 3:
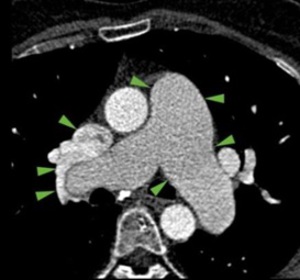
Fig. 13

Fig. 14
Fig.
13-14.
MDCT angiography : 54 years old female with Pulmonary Arterial Hypertension (PAH) and right PAPVR - upper lobar pulmonary vein flows into Superior Vena Cava (13.) and middle lobe vein flows also into SVC,
at the same place where this flows into the right atrium,
associating ASD superior cav venosus sinus type (14.) Emergency County Hospital, Radiology Department,
Cluj-Napoca/RO.
Case 4:
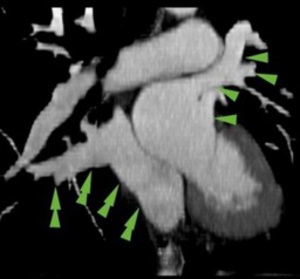
Fig. 15
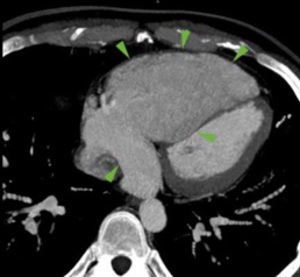
Fig. 16
Fig.
15-16 . MDCT angiography ; 27 years old patient with PAH : right PAPVR ( double arrows ) in the coronary venous sinus (15),
which is dilated (rare event) ; dilated right cavities (16).
Emergency County Hospital, Radiology Department,
Cluj-Napoca/RO.
Case 5:
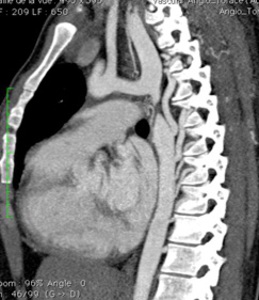
Fig. 17
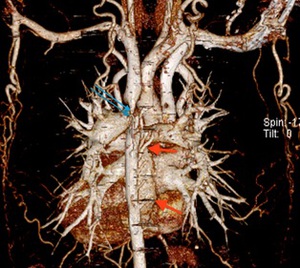
Fig. 18
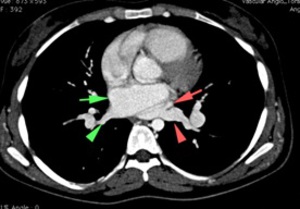
Fig. 19
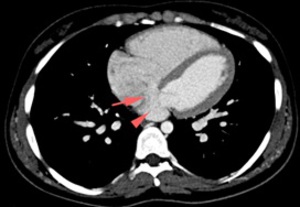
Fig. 20
Fig.
17-20.
25 years old female with tight coarctation of the thoracic aorta (17.
and 18.
Blue arrow),
which is associated with left anomalous pulmonary venous connection return,
flowing into the coronary sinus – which is enlarged,
posteriorly to the left atrium (18,
19 and 20 – red arrows ) and ASD - coronary venous sinus type (20.
Red arrow).
Emergency County Hospital, Radiology Department,
Cluj-Napoca/RO.
Case 6:
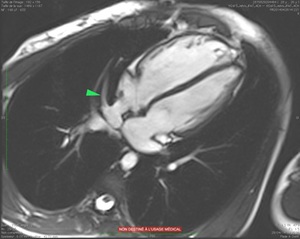
Fig. 21
Fig.
21. 26 years old male,
with PAPVC in the IVC (green arrow); Cardiac MRI-Trufisp sequence,
four cavities.
Emergency County Hospital, Radiology Department,
Cluj-Napoca/RO.






