ECR 2016 / C-1765
Paget's disease of the bone - Imaging the appendicular skeleton
This poster is published under an open license. Please read the disclaimer for further details.
Congress:
ECR 2016
Poster Number:
C-1765
Type:
Educational Exhibit
Keywords:
Diagnostic procedure, MR, Digital radiography, CT, Musculoskeletal bone, Extremities, Bones, Metabolic disorders
Authors:
G. Galea1, C. Cannataci2, C. Azzopardi3, A. Mizzi4, K. Cortis5; 1BZN1427/MT, 2 Msida/MT, 3Birkirkara/MT, 4ATTARD/MT, 5Bromley, Kent/UK
DOI:
10.1594/ecr2016/C-1765

Fig. 3:
Multimodality imaging of the lytic phase of Paget’s disease of the right...

Fig. 4:
Lateral radiograph of the right knee shows mixed osteolytic/osteosclerotic...

Fig. 5:
Anteroposterior radiograph of the pelvis shows mixed disease of the right femur...

Fig. 6:
Paget’s disease affecting the hands is rare, with hand involvement reported...

Fig. 7:
Lateral radiograph of the right calcaneum showing burnt-out Paget’s disease. ...

Fig. 8:
Anteroposterior radiograph of the right foot showing monostotic osteosclerotic...
 and lateral (bottom) radiographs of the right forearm show dense sclerosis and marked deformity of the right radius in keeping with late osteosclerotic phase Paget’s disease. Bone deformity is not exclusive to the weight-bearing limbs and may be particularly disabling in the upper limbs.")
Fig. 9:
Anteroposterior (top) and lateral (bottom) radiographs of the right forearm...
 and on bone window on axial CT (bottom). The disease is predominantly in the burnt out phase as demonstrated by the thickened, sclerotic right scapula in stark contrast to the normal left scapula.")
Fig. 10:
Paget’s disease of the right scapula and proximal humerus on anteroposterior...
 demonstrate marked deformity of the right femur on a background of mixed osteolytic/osteosclerotic Paget’s disease of the right femur. Serial, parallel, horizontal lucencies are seen in the lateral cortex of the femoral diaphysis in keeping with multiple incremental stress fractures. Whole body bone scintigraphy (right) shows the marked deformity of the right lower limb, typical uptake of Paget’s disease as well as foci of increased uptake along the lateral border of the right femur in keeping with previously described ‘pseudofractures’.")
Fig. 11:
Anteroposterior radiographs of the distal right femur and the pelvis (left and...
 and left humerus (right) show transverse fractures through the respective bones, both of which are affected by mixed lytic/sclerotic phase disease. These pathological fractures usually necessitate open reduction and internal fixation, however long-term outcome remains poor.")
Fig. 12:
Anteroposterior radiographs of the left femur (left) and left humerus (right)...

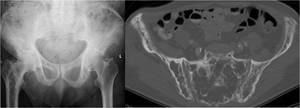
Fig. 13:
There is marked expansion of the right hemi-pelvis and right femur and the...
 and on anteroposterior radiograph (bottom). This condition is defined as intrapelvic displacement of the acetabulum and femoral head, so that the femoral head projects medial to the ischioilial line. It may be primary in origin, however in cases of Paget’s disease it is secondary to weakening of bone.")
Fig. 14:
Protrusio acetabuli secondary to Paget’s disease of the left hip is seen on...

Fig. 15:
Burnt-out Paget’s disease of the left third metacarpal is seen. Adjacent...
 and lateral (left) radiographs of the right tibia and fibula of a 75-year-old male were performed after he complained of increasing shin pain. Radiographs demonstrated burnt-out Paget’s disease with a well-defined medullary based lucency in the middle third of the tibia causing thinning of the overlying cortex. A pathological fracture (black arrow) at this location was suspected and was further evaluated by cross-sectional imaging.")
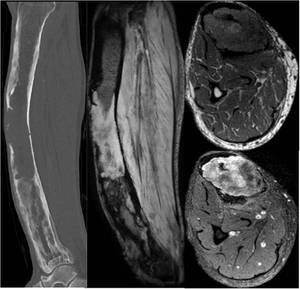
Fig. 16:
Anteroposterior (right) and lateral (left) radiographs of the right tibia and...
 confirms a lesion of soft tissue attenuation in the mid shaft of the right tibia with destruction of overlying cortex. Sagittal and axial (middle and top right) MR images show a T1-intermediate signal and T2-high signal lesion arising from the medulla of a Pagetic right tibia with oedema in the surrounding soft tissues. The lesion enhanced avidly after the administration of intravenous gadolinium (bottom right).")
Fig. 17:
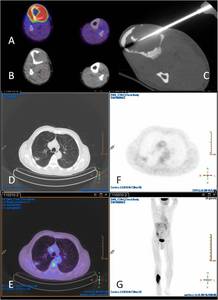
Sagittal unenhanced CT scan (left) confirms a lesion of soft tissue attenuation...
 confirmed the lesion to be highly glucose avid. CT-guided biopsy (C) and histopathological analysis revealed a pleomorphic osteosarcoma on a background of Paget’s disease of bone. PET-CT (D-G) also demonstrated lung metastases from the same lesion.")
Fig. 18:
FDG-PET CT (A & B) confirmed the lesion to be highly glucose avid. CT-guided...