ECR 2016 / C-1843
Role of Imageology in hydrocephalus. Lets innovate to understand the not so beautiful ‘Sun setting’sign!
This poster is published under an open license. Please read the disclaimer for further details.
Congress:
ECR 2016
Poster Number:
C-1843
Type:
Educational Exhibit
Keywords:
CNS, Neuroradiology brain, CT, MR, MR-Functional imaging, Diagnostic procedure, Shunts, Localisation, Cerebrospinal fluid, Dilatation, Haemodynamics / Flow dynamics
Authors:
A. V. Nair1, R. Rajeshkannan2, S. Moorthy3, P. V. Ramachandran4; 1Trivandrum, kerala/IN, 2ERNAKULAM, Ke/IN, 3Kochi/IN, 4Cochin, Kerala/IN
DOI:
10.1594/ecr2016/C-1843

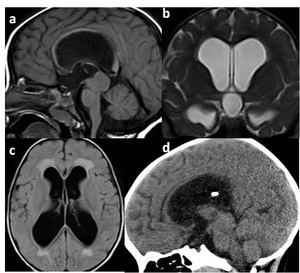
Fig. 5:
Types of Hydrocephalus
 window, Cor: Showing Comm-HCP
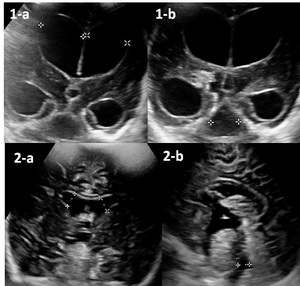
Child 2: 1year/F , H/O Meningitis 1 month back, now increasing HC
2-a, 2-b- CHILD 2:
Neurosonogram –AF window, Cor & Sag : Showing Comm-HCP
References: Dr Anirudh Nair")
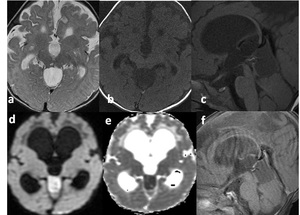
Fig. 6:
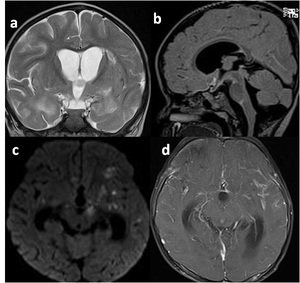
Post menignitic communicating hydrocephalus
Child 1: 5 month/M, H/O...
 T2 Cor: Hyperintense signal changes in temporal lobe bilaterally
(b) T1 Sag: Comm-HCP with prepontine hyperintensity
(c) DWI: Multiple focus of diffusion restriction-septic infarction
(d) T1 +c FS: Diffuse leptomeningeal enhancement References: Dr Anirudh Nair")
Fig. 7:
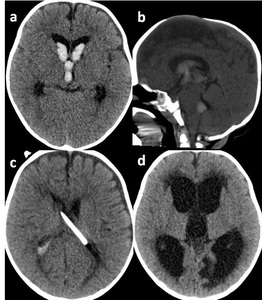
Meningo-encephalitis with Comm-HCP in 1 yr/F; Presented with fever, projectile...
 CT axial : Intraventricular hemorrhage (IVH) at lateral ventricle, foramen of monro
(b) CT Sag: IVH with bulging anterior fontanelle (AF)
(c) CT axial: Post Emergency EVD
(d) CT axial: F/up after 15 days, Comm-HCP with periventricular ooze
References: Dr Anirudh Nair")
Fig. 8:
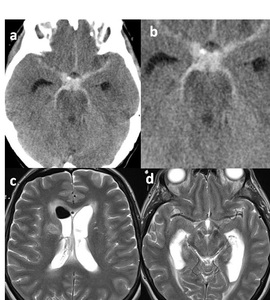
IVH with Comm-HCP in a 6 month/F , H/O fall while playing
(a) CT axial :...
 CT axial : SAH with comm-HCP; DSA showed Aneurysm at junction of right ICA-PCA
(c) MRI T2W Axial: Post EVD with Comm-HCP and ventriculocephalus
(d) MRI T2W Axial: post VP shunting 15 days after coiling . References: Dr Anirudh Nair")
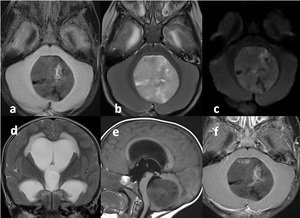
Fig. 9:
SAH due to aneurysm rupture with Comm-HCP in a 56/F , Acute onset thunderclap...
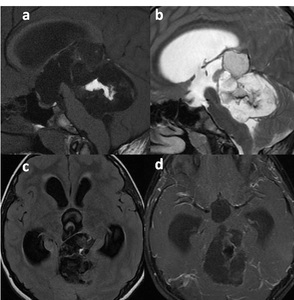
 T2 hyperintense, T1 isointense lesions at bilateral cerebellar hemispheres more towards superior aspect and vermis
(c) T2 -Cor: Dilated lateral & 3rd ventricles
(d) T1+c FS: Nodular enhancing lesions; obliteration of 4th ventricle References: Dr Anirudh Nair")
Fig. 10:
Leptomeningeal, cerebellar mets with Non-comm HCP in a 63/F, K/C/O Carcinoma ...

Fig. 11:
Normal Pressure Hydrocephalus in a 62/F, gait ataxia, dementia, dribbling of...
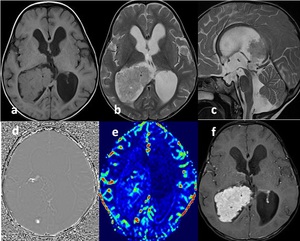
 T1W Ax: Isointense IV occipital horn lesion
(b) T2W Ax: Iso to hyperintense
(c) T2W Sag: Dilated Lateral, 3rd and 4th ventricle
(d) SWI Ax: Blooming
(e) MR Perfusion: Moderate to increased perfusion
(f) T1+C Ax: Enhancing lesion References: Dr Anirudh Nair")
Fig. 12:
Choroid plexus papilloma with Comm-HCPin a 1 year/M, Presented with bulging AF,...

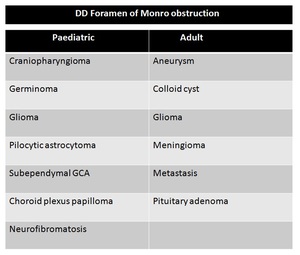
Fig. 13:
DD Foramen of monro obstruction

Fig. 14:
DD for third ventricular obstruction
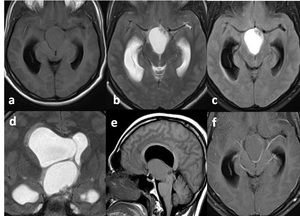
 with Non-comm HCP in a new born, antenatally detected with cystic lesion at FOM with HCP
(a) T2-Axial: Hyperintense lesion at FOM towards right frontal horn with dilated right lateral ventricle
(b) T1-Sag: Iso to hypointense cystic lesion at FOM, Normal sized 3rd , 4th ventricles
(c) T2-FLAIR: Hypointense lesion at FOM
(d) Cor-TRIM: Dilated bilateral LV (R>L) , Right temporal horn References: Dr Anirudh Nair")
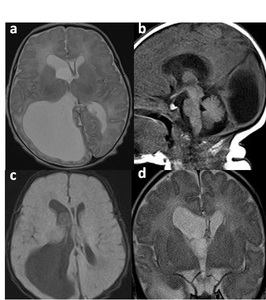
Fig. 15:
Colloid cyst at foramen of monro(FOM) with Non-comm HCP in a new born, ...
 T1 Axial: Isointense lesion
(b,c) T2 Ax, FLAIR: Hyperintense lesion with internal debris
(d) T2 Cor: Hyperintense lesion at suprasellar/FOM with LV dilatation
(e) T1 Sag: Suprasellar lesion, 3rd collapsed, 4th V normal
(f) T1 +c FS: No enhancement References: Dr Anirudh Nair")
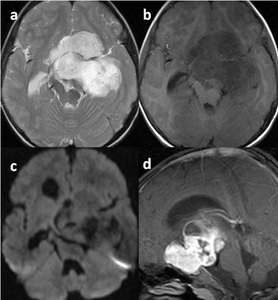
Fig. 16:
Craniopharyngioma with Non-comm HCP in a 26/M, C/O headache since 3 months...
 CT Ax: Cystic Lesion with marginal calcification; Interpeduncular extension
(b) T1W Sag: Pituitary fossa splayed with T1 iso & hyperintense areas
(c) T1+c FS- Cor: Marginal enhancement
(d) T1+C FS- Sag: Enhancing solid component in pituitary fossae, superior rim, interpeduncular cistern References: Dr Anirudh Nair")
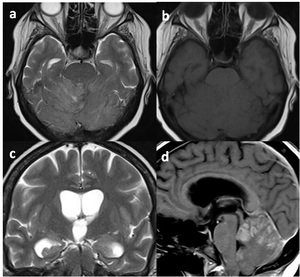
Fig. 17:
Craniopharyngioma with Non-comm HCP in a 32/M, left side visual field defect,...
 T2 Ax: Hyperintense
(b) T1 Ax: Iso to hypointense
(c) DWI: No restriction with non-communicating HCP
(d) T1+C: good enhancement References: Dr Anirudh Nair")
Fig. 18:
Pilocytic astrocytoma with Non-comm HCP in a 3yr/M presented with right sided...
 T1W Sag: T1 Hypointense lesion extending from sella into FOM
(b) T2W Sag: Heterogenously hyperintense
(c) T1W Cor: Hypointense; Non- communicating HCP
(d) T+C FS-Sag: Enhancement present References: Dr Anirudh Nair")
Fig. 19:
Recurrent pituitary adenoma in a 64/ M , S/p resection 4 years back, now...
 T1W Ax: Hyperintense
(b) T2W Ax: Hypointense
(c) GRE: No bloomimg
(d) DWI: No restriction
(e) ADC: Hyperintense
(f) T1+C FS Axial: Rim enhancement with enhancing mural nodule References: Dr Anirudh Nair")
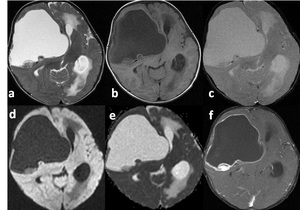
Fig. 20:
Atypical rhabdoid and teratoid tumor with non-comm HCP of left lateral...

Fig. 21:
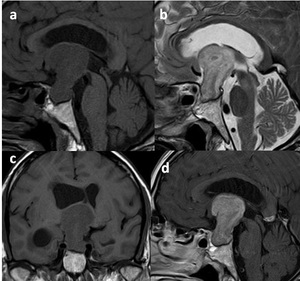
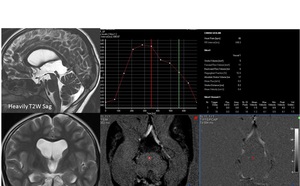
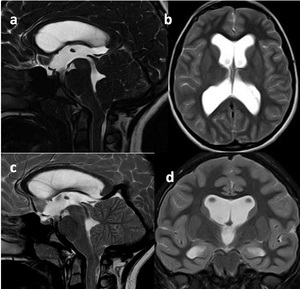
Mild functional stenosis of cerebral aqueduct in a 10/F presented with ...

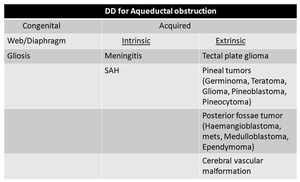
Fig. 22:
DD for aqueductal obstruction
 T1W Sag: Tectal plate is bulky, appearing isointense. Aqueduct obliterated
(b) T2W Cor: Non-communicating HCP
(c) FLAIR Ax: Periventricular seepage
(d) CT Sag: S/p VP shunt, with shunt tip in lateral Ventricle References: Dr Anirudh Nair")
Fig. 23:
Tectal plate glioma with Non-comm HCP in a 1 yr/M presented with delay in...
 T2W Ax: Hyperintense
(b) T1W Ax: Hypointense
(c) T1W Sag: Hypointense, isointense to CSF
(d,e) DWI & ADC: Diffusion restriction
(f) T1+C: Subtle internal solid component enhancement References: Dr Anirudh Nair")
Fig. 24:
Pineoblastoma with Non-comm HCP in a 4 month/M presented with history of lack...
 T1W Sag: Hyperintense streaks in center of lesion suggestive of fat
(b) T2W Sag: Hyperintense
(c) FLAIR Ax: Hypointense lesion with hyperintense internal streaks
(d) T1+C: Mild heterogenous internal enhancement References: Dr Anirudh Nair")
Fig. 25:
Pineal region teratoma with Non-comm HCP in a 17/M presented with Headache,...
 T1W Ax: Iso to hypointense
(b) T2W Ax: Hyperintense
(c) GRE: No blooming
(d) T2W Ax: CSF seeding, nodules in ependymal lining
(e) T1+C- Axial: Zuckergauss enhancement
(f) USG Spine: No focal lesion References: Dr Anirudh Nair")
Fig. 26:
Medulloblastoma with ependymal seeding and Non-comm HCP in a 29/M presented...
 T1W Ax: Hypointense
(b) T2WAx: Hyperintense
(c) DWI: Few areas of restriction
(d) T2W Cor: Non-communicating HCP with CSF seepage
(e) T1W Sag: Centered at 4th V
(f) T1+ C Ax: Minimal patchy enhancement References: Dr Anirudh Nair")
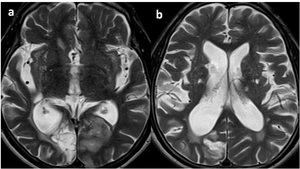
Fig. 27:
Ependymoma with Non-Comm HCP in a 1 yr/M presented with recurrent projectile...
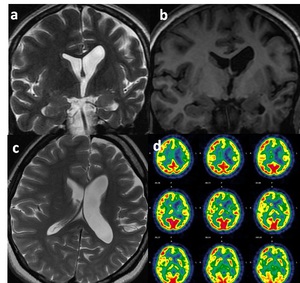
 T2 W Cor, (b) T1W Cor, (c) T1W Ax: Atrophy of left- hippocampus, mamillary body, fornix, inferior frontal gyrus, cingulate gyrus, temporal lobe, thalamus, caudate nucleus. Abnormal T2 bright signal in left hippocampus. Asymmetrical dilatation of left lateral Ventricle (LV)
(d) FDG PET: Hypometabolism on left side References: Dr Anirudh Nair")
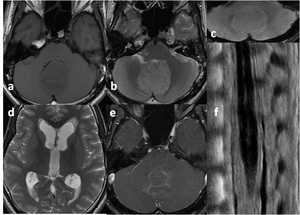
Fig. 31:
Mesial temporal sclerosis with asymmetrical left ventricular dilatation in a...
 3D CISS-Sag: Peg like hernination of cerbellar tonsil
(b) T2W Ax: Hydrocephalus
(c) T2W Sag: High velocity jet through aqueduct
(d) T2W Cor: Obstructive HCP References: Dr Anirudh Nair")
Fig. 28:
Chiari malformation type-1 with Non-comm HCP in a 14/F presented with diplopia...
: T2 Axial images showing ex vacou dilatation of right occipital horn
References: Dr Anirudh Nair")
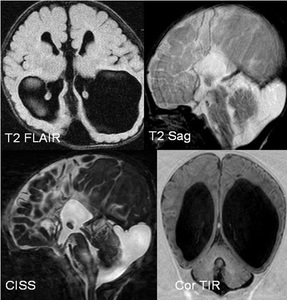
Fig. 29:
Ex vacou dilatation of right occipital horn in a 60 Yr/M presented with acute...
 FLAIR: Corpus callosal agenesis
(b) T2 Sag: Colpocephaly
(c) CISS: Hypoplastic inferior vermis
(d) Cor-TIR: Mega cisterna magna References: Dr Anirudh Nair")
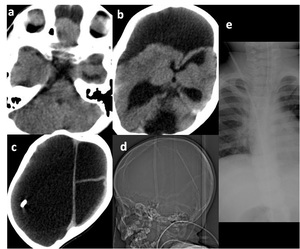
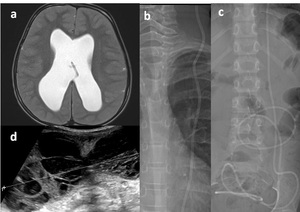
Fig. 30:
Dandy walker varient with colpocephaly in a 1 Month/M; antenatally detected...
 CT Axial- Dilated lateral ventricles, Supratentorial membraneous sac with CSF; right parietal VP shunt tip
,Left occipital lobe CSF filled area, Falx present
(d-Topogram& e- frontal Xray)
No shunt breaks/ disconnection References: Dr Anirudh Nair")
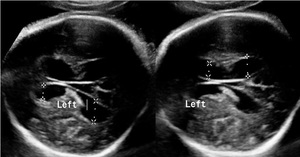
Fig. 32:
Hydrencephaly in a 1 yr/F antenatally detected with large ventricular...
 Antenatal Trancranial USG-37wks showing bilateral ventriculomegaly (>11mm) References: Dr Anirudh Nair")
Fig. 33:
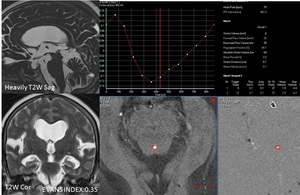
Thanatophoric dysplasia with lateral ventricular dilatation in 37 weeks GA,...
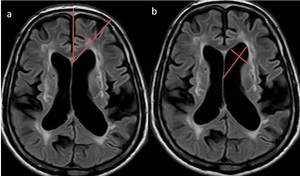
 Ventricular angle tends to be smaller in hydropcephalus than in atrophy, (b) Frontal horn radius tends to be smaller in atrophy than in hydrocephalus. References: Dr Anirudh Nair")
Fig. 37:
Cerebral atrophy in a 70 year old male;
MR axial images (a) Ventricular...
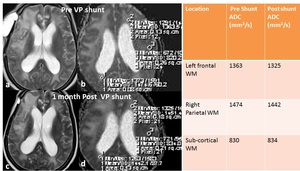
 ADC values on follow up imaging, suggestive of reduction of edema post shunting in a 57/F with history of Ca breast S/p Right temporal lobectomy for metastasis
(a,c) Dilated Ventricles, periventricular WM hyperintensity- status quo
(b,d) ADC map References: Dr Anirudh Nair")
Fig. 34:
NPH S/p VP shunt;Subtle decrease in periventricular white matter (WM) ADC...
 T2W-Ax: Hydrocephalus
(b,c) Frontal chest& Abdominal Xray: Patent shunt
(d) US- Abdomen: Septated intraperitoneal collection surrounding the shunt tip References: Dr Anirudh Nair")
Fig. 35:
VP shunt failure ; HCP with Intraperitoneal septated collection surrounding...