ANATOMY
Osseous anatomy
The wrist is a complex joint formed by 20 interdependent articulations binding 15 bones: radius and ulna,
eight carpal bones,
and the bases of 5 metacarpals.
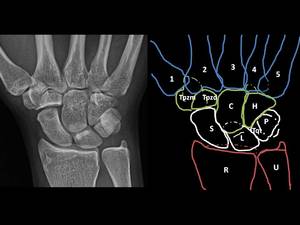
Fig. 1: From proximal to distal, radial to ulnar:
- Radius (R), ulna (U)
- Scaphoid (S), lunate (L), Triquetum (Tqt), pisiform (P)
- Traquezium (Tpzm), Trapedoid (Tpzd), capitate (C), hamate (H)
- 1st to 5th metacerpal (1 to 5)
Anatomically and functionally,
these bones are divided into proximal and distal rows:
- The distal carpal row consists of 4 tightly bound bones with little mobility between them: From radial to ulnar,
the trapezium,
trapezoid,
capitate,
and hamate.
- The proximal carpal row formed by the scaphoid,
lunate,
triquetrum and pisiform exhibits substantial intercarpal mobility.
The pisiform is a sesamoid bone providing an attachment for the the flexor carpi ulnaris and plays no role in wrist stability/kinematics.

Fig. 2: - The distal carpal row consists of 4 tightly bound bones with little mobility between them: From radial to ulnar, the trapezium (Tpzm), trapezoid (Tpzd), capitate(C), and hamate (H).
- The proximal carpal row formed by the scaphoid (S), lunate (L), triquetrum (Tqt) and pisiform (P) exhibits substantial intercarpal mobility.
The complex motions of the wrist occur through three joints: radiocarpal,
midcarpal,
and carpometacarpal.
- The radiocarpal joint is an oval-shaped glenoid articulation formed by the distal articular surface of the radius and triangular fibrocartilague complex (TFCC),
and the convexities of the scaphoid,
lunate and triquetum bones.
- The midcarpal joint is a combination of three types of articulations:
- Radial column: On the radial side,
formed by the scaphotrapeziotrapezoid space
- Central column: consist of the scaphocapitate and the lunocapitate space
- Ulnar column: On the ulnar side,
formed by the triquetral-hamate space

Fig. 3: - Radial column: scaphotrapeziotrapezoid space
- Central column: scaphocapitate and the lunocapitate space
- Ulnar column: triquetral-hamate space
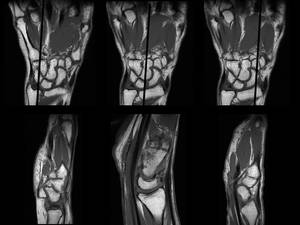
Fig. 4: Coronal and sagital T1WI representation of the bones involved in each midcarpal joint articulation:
Left - Ulnar column: triquetral-hamate
Middle image - Central column: scaphoid-capitate and lunate-capitate
Right - Radial column: scaphoid-trapezio-trapezoid
Ligamentous anatomy
Multiple ligaments help stabilize the wrist to the forearm and hand.
Most of the wrist ligaments are intracapsular,
except for the transverse carpal ligament and two ligaments attaching to the pisiform to the hook of the hamate and to the base of the fifth metacarpal (i.e.,
pisohamate and pisometacarpal ligaments).
There are two categories of intracapsular ligaments:
- The extrinsic ligaments attach the forearm bones (i.e.
radius and ulna) with the carpal bones
- The intrinsic ligaments form connections between carpal bones
The extrinsic ligaments are stiffer,
while the intrinsic ligaments are capable of greater elongation.
Likewise,
the volar ligaments are stronger than the dorsal ligaments.
Extrinsic Ligaments
1.
Extrinsic Palmar Ligaments
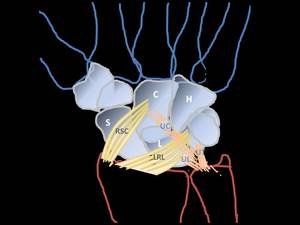
Fig. 6: EXTRINSIC PALMAR LIGAMENTS
Palmar Radiocarpal ligaments
- radioscaphocapitate ligament (RSC)
- long radiolunate ligament (LRL) or radiolunotriquetral
Ulnocarpal complex
- ulnocapitate (superficial) (UC)
- ulnolunate ligament (UL)
- ulnotriquetral (UT)
Θ Radial collateral ligament
Θ Palmar Radiocarpal ligaments
- radioscaphocapitate ligament (RSC)
-
- runs from volar aspect of radial styloid process and inserts into palmar side of capitate,
creating a a fulcrum over which the scaphoid rotates
- acts as primary stabilizer of the wrist after PRC and prevents ulnar drift
- long radiolunate ligament (LRL) radiolunotriquetral
-
- parallel to radioscaphocapitate ligament,
runs from the palmar rim of the distal part of the radius to the radial margin of palmar horn of lunate;
- counteracts ulnar-distal translocation of the lunate
- radioscaphoid (RS),
- radioscapholunate ligament (ligament of Testut and Kuenz): Embryologic neurovascular remnant with no mechanical strenght
- short radiolunate ligament
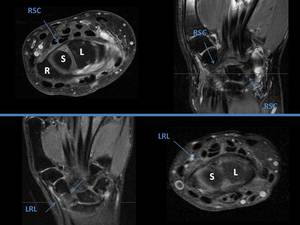
Fig. 7: Axial and coronal MRI repesentation of the radioscaphocapitate (RSC) and radiolunotriquetral / long radiolunate ligament (LRL)ligaments
♦ Space of Poirier
Central weak area of the wrist in the floor of the carpal tunnel at the level of the proximal capitate,
between the palmar radioscaphocapitate ligament and palmar long radiolunate ligament;
In perilunate dislocations this space allows the distal carpal row to separate from the lunate; in lunate dislocations,
the lunate escapes into this space
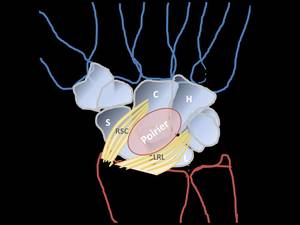
Fig. 8: Space of Poirier is a central weak area of the wrist in the floor of the carpal tunnel at the level of the proximal capitate between the volar radioscaphocapitate ligament and volar long radiolunate ligament.
- Ulnocarpal complex
- ulnocapitate (superficial) (UC),
- ulnolunate ligament (UL),
- this is a key ligament along w/ the
 TFC
TFC
- ulnotriquetral (UT)
- triangular fibrocartilage complex
2.
Extrinsic Dorsal Ligaments less important
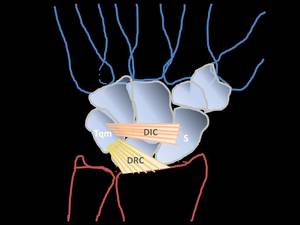
Fig. 9: EXTRINSIC DORSAL LIGAMENTS
- Radiotriquetral / Dorsal radiocarpal ligament (DRC)
- Dorsal scaphotriquetral / Dorsal intercarpal ligament (DIC)
Θ Dorsal radiocarpal ligament (DRC)
- Key ligament in preventing volar intercalated segment instability (VISI)
-
- originates on the radius and has minor attachments to the lunate,
with the bulk of the attachment on the triquetrum
- helps stabilize the lunate from volar flexion and is also a passive pronator of the wrist
Θ Dorsal intercarpal ligament (DIC)
- Crossing from the proximal row to the distal row (scaphoid to capitate and triquetrum).
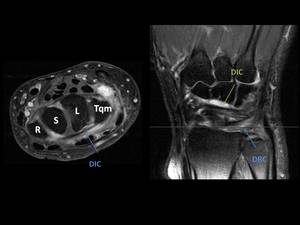
Fig. 10: Axial and coronal DP Fat Sat. Dorsal radiocarpal ligament (DRC)
Intrinsic (Interosseous) Ligaments
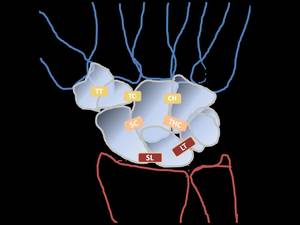
Fig. 11: INTRINSIC (INTEROSSEOUS) LIGAMENTS
.Proximal row
- scapholunate interosseous ligament (SLIL)
- lunotriquetral interosseous ligament (LTIL).
.Distal row
- trapeziotrapezoid ligament
- trapeziocapitate ligament
- capitohamate ligament
.Palmar midcarpal
- scaphocapitate (SC)
- triquetral –hamate-capitate (THC)
1.
Proximal row
Θ scapholunate interosseous ligament (SLIL)
- primary stabilizer of scapholunate joint: its injury can result in one of most common causes of carpal instability: scapholunate dissociation.
- 3 components
-
- dorsal portion (dSLIL): thickest and strongest
-
- volar portion (pSLIL),
-
- proximal portion
-
- made up of fibrocartilage and has no significant strength
- disruption leads to lunate extension when the scaphoid flexes creating DISI deformity

Fig. 12: Scapholunate interosseous ligament (SLIL): Coronal and axial DP FS showing its dorsal (dSLIL) and volar portion (pSLIL).
Θ lunotriquetral interosseous ligament (LTIL).
-
- also composed of 3 components: dorsal,
volar and proximal
- Unlike the SLIL,
here the volar component is the strongest.
- disruption leads to lunate flexion when the scaphoid is normally aligned creating VISI deformity (in combination with rupture of dorsal radiotriquetral rupture)
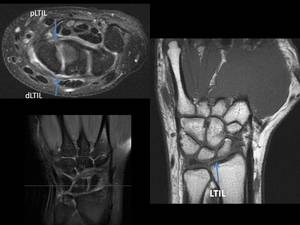
Fig. 13: Linotriquetal interosseous ligament (LTL): Coronal DP FS and T1WI and axial DP FS showing its dorsal (dLTIL) and palmar portion (pLTIL).
The proximal aspect of both ligaments is thin and membranous and does not contribute to intercarpal stability.
When intact,
these two ligaments separate the radiocarpal and midcarpal compartments of the wrist.
2.
Distal row
- trapeziotrapezoid ligament
- trapeziocapitate ligament
- capitohamate ligament
Particularly important in the protection of the carpal tunnel contents.
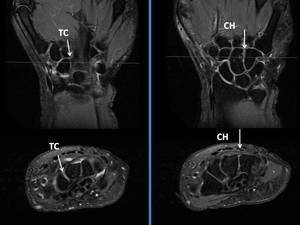
Fig. 14: Coronal and axial DP FS views showing distal carpal row interosseous ligaments.
On the left, trapeziocapitate (TC) ligament
On the right, capitohamate (CH) ligament
3.
Palmar midcarpal
- scaphocapitate (SC)
- triquetral –hamate-capitate
Together they bridge the midcarpal joint as the arcuate or "Deltoid" ligament or long palmar intrinsic ligament
CARPAL KINEMATICS
The distal row of bones (trapezium,
trapezoid,
capitate and hamate) is tightly bound by intercarpal ligaments,
allowing for minimal motion between them. Similarly,
the distal radius and ulna,
although they move in pronation and supination,
are essentially stable.
However,
the proximal row of the carpus (scaphoid,
lunate,
and triquetram) is an intercalated segment with no muscle insertions; its stability depends entirely on the capsular and interosseous ligaments between them and their movement is dictated by the surrounding articulations.

Fig. 15: Intercalated segment of the wrist (red) composed by the bones on the proximal row of the carpus (scaphoid, lunate, and triquetram).
These bones have no muscle insertions and their movement is dictated by the surrounding articulations.
Over the past several decades,
many theoretical models have been described to explain the complexities of carpal motion.
The oval-ring oval ring concept suggested by David Lichtman functionally depicts the carpus as a transverse ring formed by 2 rows of bones,
proximal and distal,
joined by two physiologic links: the mobile scaphotrapeziotrapezoid (STT) joint (radial link) and the rotary triquetrohamate (TqH) joint (ulnar link).
These links create reciprocal motion between the proximal and distal carpal rows.
In radial deviation the proximal carpal row flexes and the scaphoid moves out of the way to allow the trapezoid/ trapezium to move radially.
In ulnar deviation,
the proximal carpal row extends,
and the triquetrum moves out of the way to allow the hamate to move ulnarly.
These movements allow the so-called “dart-throwing” motion (radiodorsal to ulnopalmar),
which combines radial and ulnar translocation of the proximal carpal row with flexion and extension at the radiocarpal joint.
Any injury or disease modifying bone geometry,
articular inclination,
ligament integrity,
or muscle function may alter carpal motion,
leading to carpal instability.
CLINICAL EVALUATION
Patients presenting with carpal instability may or may not have had a prior traumatic event. When present,
the most common injury mechanism is from a fall on an outstretched hand with wrist extended.
Violent trauma such as a motorcycle accident or a contact sports injury is also a frequent cause of carpal instability.
When a ligamentous wrist injury occurs,
patients will generally describe one or more of the following symptoms:
- Wrist pain with motion
- Loss of grip strength: <50% of contralateral grip strength is pathognomic
- Swelling and tenderness
- A "clunk,
snap,
or click" during use (it may or may not be painful)
Unfortunately,
there are no pathognomonic clinical features that are diagnostic of carpal instability.
The symptoms are often subtle and unimpressive
In many cases,
carpal ligament injuries are associated with fractures of the adjacent bones.
For instance,
distal radius fractures are commonly seen with scapholunate ligament injury.
Therefore,
it is important to survey the entire overall spacial relationship of the carpal bones,
in addition to assessing the more obvious fracture(s).
DIAGNOSTIC TESTS
The first diagnostic approach in the study of carpal instability is the conventional X-ray which should include at least a posteroanterior (PA) view in neutral rotation and lateral view.
PA radiograph
Useful to assess Gilula's lines and the scapholunate gap.
o Gilula's lines represent the arcs of the wrist:
- along the proximal aspect of the proximal row of carpal bones;
- along the distal aspect of the proximal row of carpal bones;
- along the proximal convex curvature of the capitate and hamate.
Disruption of these arcs,
or any overlapping of adjacent bones,
commonly indicates underlying carpal instability or fracture.
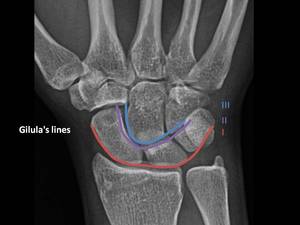
Fig. 16: Gilula's lines:
- along the proximal aspect of the proximal row of carpal bones (I - red)
- along the distal aspect of the proximal row of carpal bones (II - purple)
- along the proximal convex curvature of the capitate and hamate (III - blue)
Disruption of these arcs, or any overlapping of adjacent bones, commonly indicates underlying carpal instability or fracture.
o The scapholunate gap should measure less than 3mm.
A distance greater than 5mm is highly suggestive of rupture of the scapholunate ligament (Terry Thomas sign).

Fig. 17: The normal scapholunate gap should measure less than 3mm. A distance greater than 5mm is highly suggestive of rupture of the scapholunate ligament (Terry Thomas sign).
o The intercarpal joints are profiled,
parallel,
and of similar width (1–2 mm)
o Medially the radius articulates with the head of the ulna at the ulnar notch.
The head of the ulna is usually 2mm shorter than the radius and either touches or slightly overlaps the radius at the distal radioulnar joint.
However,
obtaining a PA view that clearly shows the scapholunate gap without some bony overlap can be difficult; in that case we may need to resort to additional views such as a PA Clenched view or PA in maximum ulnar deviation.
Also,
findings should always be compared side to side to account for interpersonal variability.
Lateral radiograph 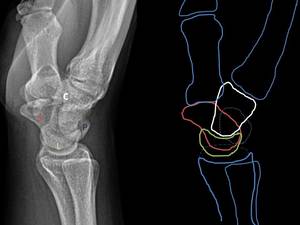
Fig. 5: Lateral radiograph of the wrist: normal anatomy
Θ Articular surfaces of radius,
lunate and capitate and third metacarpal should be in a straight line along their longitudinal axes and be congruent (parallel).
Θ The lateral view is useful to assess the scapholunate and capitolunate angles.
- Scapholunate angle: constructed by the intersection of a line drawn parallel to the long axis of the scaphoid and a line drawn perpendicular to the AP axis of the lunate.
Range between 30-60 degrees.
>70° confirms SL instability
- Capitolunate angle: constructed by the intersection of a line drawn parallel to the long axis of the capitate and a line drawn perpendicular to the AP axis of the lunate.
It shold measure less than 30 degrees in resting position.

Fig. 18: - Scapholunate angle (left): intersection of a line drawn parallel to the long axis of the scaphoid and a line drawn perpendicular to the AP axis of the lunate. Normal range between 30-60º.
- Capitolunate angle (right): intersection of a line drawn parallel to the long axis of the capitate and a line drawn perpendicular to the AP axis of the lunate. It should measure less than 30º in resting position.
If the lunate is dorsiflexed more than 15º than the capitate on lateral radiography,
a diagnosis of a dorsal intercalated-segment instability (DISI) deformity is confirmed,
associated with scapholunate instability.
Conversely,
a lunate volarly flexed more than 15º defines a volar intercalated-segment instability (VISI),
associated with lunotriquetral instability.
If the diagnosis remains doubtful,
it is advisable to resort to other diagnostic imaging studies including CT scanning,
indispensable for the detection of hidden fractures; and especially MRI,
which is recommended for the in-depth study of the fibrocartilaginous and ligamentous structures
Other imaging techniques are bone scan,
useful to localize the site of acute injury (eg occult fractures),
fluoroscopy and arthroscopy; the latter considered the gold standard for anatomic and functional examination
CLASSIFICATION
Multiple schemes for classification of carpal instability patterns had been developed.
Perhaps the most widely adopted is the Mayo Classification.
This scheme classifies carpal instability into four major categories:
1.
Dissociative Carpal Instability (CID):
~ Instability within the interossoeus ligaments;
a.
Proximal Dissociative Carpal Instability (DISI and VISI)
1.
scapholunate dissociation
2.
lunotriquetral dissociation
b.
Distal Dissociative Carpal Instability
2.
Non-Dissociative Carpal Instability (CIND):
~ Instability between rows / of a carpal row as a whole;
a.
radiocarpal CIND
b.
midcarpal CIND
3.
Carpal Instability Complex (CIC):
~ Combinations of CID and CIND,
or instability within and between rows;
a.
Perilunate dislocation
b.
Others
4.
Adaptive Carpal Instability (CIA)
~ secondary malposition of the carpus which results from a non-union or malunion of the distal radius or carpal bones.
a.
Malposition of carpus with distal radius malunion
b.
Malposition of carpus with scaphoid non-union
c.
Malposition of carpus with lunate malunion
d.
Malposition of carpus with Madelung’s deformity
1. Dissociative Carpal Instability
Instability secondary to a true disruption between carpal bones of the same row due to the rupture of interosseous ligaments,
as a result of well-healed displaced carpal skeletal fractures or badly healed fractures (pseudoarthrosis)
The proximal carpal row is the most commonly affected.
The carpal mal-alignment results in increased stresses on the radio-scaphoid and capito-lunate joints
a.
Proximal row Dissociative Carpal Instability (DISI and VISI)
• SCAPHOLUNATE DISSOCIATION: DISI pattern
Scapholunate instability is the most common form of carpal instability.
It may be the result of traumatic injuries to the SL ligament (the most common cause,
the injury usually occurs with wrist positioned in extension,
ulnar deviation and carpal supination),
also unstable scaphoid fractures,
rheumatoid arthritis,
calcium pyrophosphate deposition disease,
and Kienböck’s disease.
The spectrum of presentation is broad and can be conceptualized in the form of a staging scheme of progressive severity.
1.
“Occult” or “pre-dynamic” SL instability results from a partial SL ligament tear.
Routine and stress radiographs are normal,
and the use of MRI or MR arthrography is necessary to assess partial SL ligament tears.

Fig. 19: "Occult” or “pre-dynamic” SL instability.
Routine (upper left) and stress radiographs are normal.
Axial fat-satturated DP demonstrate a disruption of the scapholunate ligament (blue arrows), with surrounding soft tissue oedema.
2.
On “dynamic” SL instability the SLL is completely disruptured; however,
the stabilizing extrinsic ligaments remain intact.
Routine radiographs are still usually normal but the instability becomes evident in stress views.
Diastasis of the SL interval can be seen on the clenched fist,
or radial–ulnar deviation views.

Fig. 20: “Dynamic” SL instability.
Routine radiographs are usually normal (left) but the instability becomes evident in stress view such as clenched fist or radial–ulnar deviation views (PA clenched fist view - right)
3.
Complete tear of the SL ligament along with injuries to the secondary stabilizing ligaments,
results in static SL instability.
The scaphoid and lunate rotate in opposite directions.
There is flexion of the distal pole of the scaphoid (‘rotatory subluxation of the scaphoid’ or stage I of the Mayfield classification of perilunar instability).
The unconstrained lunate rotates dorsally,
while there is a midcarpal subluxation of the capitate at the posterior horn of the lunate.
The zigzag deformity that develops in the middle carpal column is known as the “dorsiflexed intercalated segment instability” (DISI).
Classic signs of SL dissociation are evident on routine wrist x-ray views.
– PA radiograph
o the flexed scaphoid has a foreshortened appearance with the so-called “cortical ring” sign (the cortical outline of the distal pole of scaphoid is seen in cross section)
o Lunate may have a triangular appeareance
o Disruption of Gilula’s arcs I/II as the scaphoid migrates proximally;
o scapholunate gap over 3 mm (Terry Thomas sign) is suspicious for DISI.
Nonetheless,
when in doubt it is useful to compare this gap to the opposite wrist.
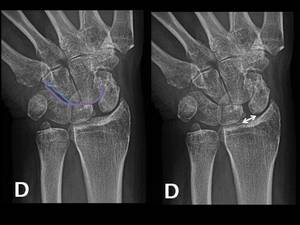
Fig. 21: "Static SL instability".
PA radiograph showing disruption of Gilula’s arcs I/II and scapholunate gap over 3 mm (Terry Thomas sign), suspicious for DISI.
– Lateral radiograph
o palmar flexion of the scaphoid and dorsiflexion of the lunate.
o scapholunate angle (formed by intersection of longitudinal axes of the scaphoid and lunate,
normal 30-60º) increased over 70° is the most evident sign of SLD.
o Radiolunate angle greater than 15 degrees of extension
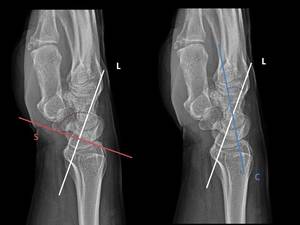
Fig. 22: "Static SL instability". Lateral radiograph shows:
- Scapholunate angle (left- red) increased over 70°. This is the most evident sign of SLD.
- Capitolunate angle (right - blue) greater than 15 degrees
If untreated,
SL instability progresses to degeneration and collapse of the carpus,
known as scapholunate advanced collapse (SLAC).
Cartilage degeneration,
chondritis of the articular facets,
reduction of the joint space and formation of osteophytes may be seen.
The progression involves a number of subsequent stages of increasing severity:
Initially,
osteoarthritic changes are limited to the radial styloid–scaphoid portion of the radioscaphoid joint (SLAC I),
progressing to involve the entire radioscaphoid joint (SLAC II),
the midcarpal joint at the scaphocapitate and/or capitolunate articulations (SLAC III),
and eventually the whole carpus (SLAC IV).
In this last stage,
the capitates migrates proximally into the scapholunate gap and approaches the radius while the lunate assumes a dorsiflexed position.
The midcarpal joint collapses under compression.
Carpal instability arising from a nonunion scaphoid fracture can progress to pancarpal arthrosis through relatively similar degenerative stages,
known as “scaphoid nonunion advanced collapse” (SNAC).

Fig. 24: Coronal T1WI demonstrates the presence of several osteoarthritic such as chondritis of the articular facets and reduction of the joint space changes involving the entire radioscaphoid joint (SLAC II)
PA radiograph
Carpal height can be used to quantify carpal collapse and determine disease.
On a PA radiograph,
carpal height is the distance between the third metacarpal base and the distal radial articular surface.
The carpal height ratio is the carpal height divided by the third metacarpal length,
with normal values of 0.54± 0.03.
The carpal height index is an intrapersonal value obtained by dividing the carpal height ratio of the diseased wrist by that of the normal wrist,
with normal values of 1.000 ± 0.015.
it doesn’t allow comparison among individuals.
MR Imaging:
MRI allows the visualization of the radiologically “silent” instability stages I and II of SLD.
In T2-weighted sequences,
SLL disruption is identified an absent ligament or a hyperintense fluid accumulation adjacent to the ligamentary flaps.
Coronal as well as transaxial slices are mandatory to fully visualize the altered SLL.
Accuracy rates of plain MRI have been reported in ranges between 50 and 80%

Fig. 23: Axial and coronal DP FS demonstrate the disruption of the scapholunate ligament,with a hyperintense fluid accumulation adjacent to the ligamentary flaps.
The application of intravenous contrast agent increases the accuracy of MRI.
In ligamentary tears,
there is an enhancement at the rupture site caused by an intense hyperemia of synovial and fibrovascular tissue.
This regeneration process develops focally at the tear immediately after the injury and is seen in contrast-enhanced MRI up to 9 months.
• LUNOTRIQUETAL DISSOCIATION: VISI pattern
The lunotriquetral (LT) instability is less common than the SL ligament dissociation.
Usually,
an isolated rupture of the intrinsic lunotriquetal ligament causes no symptoms.
The adjacent extrinsic (scaphotriquetral,
ulnotriquetal y dorsal radiocarpal) ligaments must also be injured to produce complete lunotriquetral instability with pain at the ulnar side of the wrist and a motion-associated click phenomenon.
The mechanism of injury is variable and includes traumatic event,
typically forced extension or extension - radial deviation; but also attrition by age,
positive ulnar variance,
and perilunate (or reverse perilunate) injuries.
Initially,
the flexion of the scaphoid induces volar flexion of the lunate relative to the longitudinal axis of the radius and capitate,
while the triquetrum remains linked to the hamate in supination and extension; as the injury advances, volar intercalated segment instability (VISI) deformity develops.
X-rays:
- often radiographs will be unremarkable in lunotriquetral instability;
PA View:
– disruption of Gilula’s arcs by a step off between lunate and triquetrum
– proximal migration of the triquetrum and/or LT overlap
– the lunate may demonstrate a triangular shape.
– scaphoid volar flexed and shortened
– triquetrum is dorsiflexed and distal in relation to the hamate;
– unlike scapholunate dissociation,
LT diastasis is rarely observed on PA radiographs

Fig. 25: PA View findings on VISI:
- triangular shape of the lunate.
- disruption of Gilula’s arcs by a step off between lunate and triquetrum.
Lateral view:
– volar tilt of the lunate and scaphoid with +/- 30 deg volar tilt
– dorsal tilt of the capitates
– increased capitolunate angle,
> 15º of flexion (lunate and capitate normally co-linear)
– decreased scapholunate angle,
less than 30º (normal is 47°).
– If the lunate and triquetrum can be seen,
the normal luno-triquetral angle of ~ -16 degrees becomes neutral or positive

Fig. 26: Lateral view findings on VISI:
- on the left, decreased scapholunate angle, less than 30º
- on the right, increased capitolunate angle, > 15º of flexion
- volar tilt of the lunate and scaphoid
While DISI deformity is always a pathologic condition,
VISI may occasionally be seen in uninjured wrists in patients with ligamentous laxity.
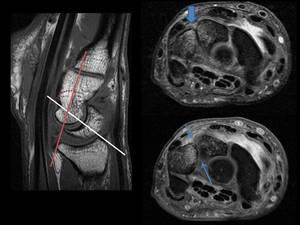
Fig. 27: Sagital T1WI demontrates the volar tilt of the lunate and consequently increased capitolunate angle .
Axial fat satturated DP shows bone marrow edema on both lunate and triquetum and absent lunotriquetal ligament.
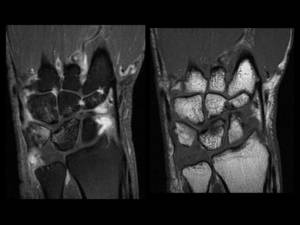
Fig. 28: Coronal DP FS and T1WI views demonstrate LT ligament disruption, with an increased lunotriquetal space on the proximal aspect of the articulation.
b.
Distal row Dissociative Carpal Instability (CID): axial instability
Axial dissociation of the carpus is a traumatic longitudinal disruption of the ligaments of the distal carpal row.
Since this bones are tightly bound by intercarpal ligaments,
distal carpal row dissociations are rare,
typically result from blast or crush injuries,
and are usually associated with fractures and extensive soft-tissue injuries.
Axial dissociations may occur on both the radial or ulnar side of the wrist and may be classified into three groups: axial ulnar disruption,
axial radial disruption,
and combined disruptions.
Nomenclature: the prefix “peri” indicates that the dislocation is around a bone,
and “trans” denotes that the dislocation is associated with a fracture through that bone.

Fig. 29: Non-dissociative Carpal Instability (CIND) Ilustrated, purely ligamentous axial radial and ulnar dislocations.
(A) Peritrapezoid and peritrapezium axial radial dislocation. With axial radial dislocation, the distal carpus splits longitudinally into two columns: the ulnar column (light blue) is stable with regard to the radius, and the radial column(dark blue) displaces most commonly in the radial and proximal direction.
X-ray sowing a tras-trapezium axial radial dislocation.
(B) Perihamate peripisiform axial ulnar dislocation. In ulnar disruptions, the radial column (light blue) is stable with regard to the radius, and the ulnar column (dark blue) displaces most commonly in the ulnar and proximal direction.
2. Non-dissociative Carpal Instability (CIND)
It consists on an alteration in the articular relationship either between the forearm and the proximal carpal row (radiocarpal CIND) or between the proximal and distal rows (midcarpal CIND),
while the joint connections between the skeletal elements of each row are maintained.
CIND is frequently encountered in young people and is thought to be due to congenital ligamentous laxity,
traumatic defects of the extrinsic carpal ligaments or malunited distal radial fracture
X-rays:
- palmar translation of the carpi on the radius may often show VISI deformity;
- less often dorsal translation of the carpi may produce a DISI deformity;
a) RADIOCARPAL CIND
Under physiological conditions,
the extrinsic carpal ligaments resist the tendency of the carpus to slide down the ulnar and palmar tilts of the distal radius.
Injury of these ligaments may predispose to radiocarpal instability and ulnar translocation of the carpus.
Abnormal translation of lunate in ulnar direction is pathognomonic of ulnar translocation.
Taleisnik described two different patterns of ulnar translocation according to position of scaphoid:
~ The entire carpus migrates in ulnar direction along the normal slope of the distal radius (type I).
There is a resultant widening (more than 2 mm) of the distance between the radial styloid process and the scaphoid,
while the radiolunate contact is less than 50%.
~ When the radial extrinsic ligaments are intact,
the scaphoid remains in place,
whereas the lunate–triquetrum block translocates in the ulnar direction,
causing an scapholunate diastasis (type II).
This latter type is a combined CIND and CID pattern,
considered a “carpal instability complex” subcategory.

Fig. 30: Radiocarpal translocation instability.
(A) Ulnar translocation of the wrist (Taleisnik’s type I). X-ray sohws a widened radioscaphoid joint as well as decreased radiolunate contact length.
(B) Radial translocation of the wrist as a sequel of a malunited distal radius fracture. The ulnar inclination of the radius is pathologically reduced, and the radiolunate contact diameter is increased.
b) MIDCARPAL CIND
Of all the forms of carpal instability,
midcarpal instability (MCI) has been the most confusing,
with poorly understood etiology and pathomechanics.
Many patients with midcarpal CIND have joint hypermobility with ligamentous laxity and no history of trauma.
There is no clear agreement on a classification for patterns of MCI,
with overlapping descriptions in the literature.
There appear to be two fundamental patterns of MCI (ulnar and radial) from palmar ligament damage,
with a third that demonstrates combined features of the two.
The is also a last type of MCI from dorsal ligament damage
X-rays:
Lateral view
- The lunate is subluxated volarly from the radius but not completely dislocated.
- The capitate is dislocated from the lunate but not as dorsally as seen in a perilunate dislocation.
Ulnar Deviation Lateral View:
- normally ulnar deviation will cause the lunate to dorsiflex and shift volarly,
and the radio-luno-capitate alignment resembles a DISI pattern
- volar shift of the lunate helps maintain the normal co-linear relationship of the radius and the capitate;
- on mid carpal ulnar instability the lunate will dorsiflex,
but will not have normal palmar translation;
- hence,
the longitudinal axis of the capitate lies above the axis of the radius; "zig zag" deformity
3.
Complex Carpal Instability (CIC)
CIC refers to injury patterns in which there is an association of dissociative and non-dissociative instability; perilunate dislocation being a typical example.
Perilunate dislocation result from high-energy loads that lead to ligament injury,
typically secondary to forced wrist extension,
ulnar deviation and midcarpal supination.
These injuries were first described by Mayfield,
who classified them by sequential ligament injury from radial to ulnar.
- Stage I refers to injury to the scapholunate ligament with partial disruption (SL dissociation or rotatory subluxation of the scaphoid).
This stage is categorized as dissociative carpal instability - CID.
- In stage II there is complete scapholunate disruption with dislocation of the capitate,
usually dorsally.
- In stage III (perilunate dislocation) there is lunotriquetral ligament disruption with scapholunate and capitolunate dissociations.
Occurs when the lunate maintains its normal position in the lunate fossa of the radius while all other carpal bones are dislocated posteriorly.
- Finally,
stage IV (lunate dislocation) includes rupture of the dorsal radiocarpal ligament allowing the lunate to dislocate in a volar direction with up to 90 degrees rotation,
while the capitate drops proximally into space vacated by lunate and becomes aligned with the radius.
X-rays:
– The PA view X-ray will show an interruption in the second Gilula’s arc,
consequent to the altered lunate tilt.
The lunate appears has a triangular appearance and overlaps the capitate
– The lateral view X-ray shows an alteration of the normal alignment between the distal surfaces of the radius,
lunate,
capitate and third metacarpal.
- In the case of perilunate dislocation,
the radiolunate articulation is preserved and the rest of the carpus is displaced dorsally.
There is an reduced scapholunate angle (normal 30-60 degrees) and an increased capitolunate angle (normal 0-15 degress)

Fig. 31: PERILUNATE DISLOCATION Mayfield stage 3
Triangular shape of the lunate on PA view.
The lateral view shows all other carpal bones dislocated posterior with respect to lunate (red outline).

Fig. 32: PERILUNATE DISLOCATION
Left- reduced scapholunate angle (normal 30-60 degrees)
Right- increased capitolunate angle (normal 0-15 degress)
- In lunate dislocations,
the lunate is displaced and rotated volarly while the rest of the carpal bones are in a normal anatomic position in relation to the radius.

Fig. 34: LUNATE DISLOCATION. Mayfield stage IV
On the lateral radiograph the lunate is displaced and rotated in a volar direction. The rest of the carpal bones are in a normal anatomic position in relation to the radius.
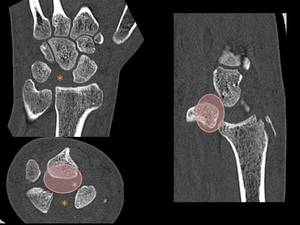
Fig. 35: LUNATE DISLOCATION. Mayfield stage IV
CT imaging shows the dislocation of the lunate in volar direction into the space of Poirier (red oval)

Fig. 36: LUNATE DISLOCATION. Mayfield stage IV
TC 3D imaging
The Mayfield classification refers to lesser arc injuries where there is only ligamentous injury.
When there is superimposed fracture of the bones surrounding the lunate,
the injury is referred to a “greater arc injury” or a perilunate fracture dislocation.
The most common greater arc injury is the trans-scaphoid perilunate dislocation

Fig. 33: TRANS-SCAPHOID PERILUNATE DISLOCATION. Mayfield stage 3
Triangular shape of the lunate on PA view.
The lateral view shows a normal relation of the lunate with respect to the distal radius with posterior dislocation of the remaining carpal bones.
Scaphoid fracture (green outline) may be seen asociated to the dislocation.
CIC also includes type II radiocarpal instability,
where there is translocation of the lunate–triquetrum block in ulnar direction while the scaphoid remains associated with the distal radius,
leading to scapholunate dissociation.
4. Adaptive Carpal Instability (CIA),
This category of instability presents as an adaptive change of the carpus secondary to malunited or non-united fractures on the distal radius or carpal bones,
but may also occur as a result of Madelung’s deformity.
The process can progress to intrinsic ligament failure by attrition.

Fig. 37: Adaptive Carpal Instability (CIA), secondary to malunited fracture on the distal radius.

Fig. 38: Adaptive Carpal Instability (CIA), secondary to non-united scaphoid fracture.

, ulna (U)
- Scaphoid (S), lunate (L), Triquetum (Tqt), pisiform (P)
- Traquezium (Tpzm), Trapedoid (Tpzd), capitate (C), hamate (H)
- 1st to 5th metacerpal (1 to 5)")
, trapezoid (Tpzd), capitate(C), and hamate (H).
- The proximal carpal row formed by the scaphoid (S), lunate (L), triquetrum (Tqt) and pisiform (P) exhibits substantial intercarpal mobility.")




- long radiolunate ligament (LRL) or radiolunotriquetral
Ulnocarpal complex
- ulnocapitate (superficial) (UC)
- ulnolunate ligament (UL)
- ulnotriquetral (UT)")
 and radiolunotriquetral / long radiolunate ligament (LRL)ligaments")


- Dorsal scaphotriquetral / Dorsal intercarpal ligament (DIC)")
")
 LIGAMENTS
.Proximal row
- scapholunate interosseous ligament (SLIL)
- lunotriquetral interosseous ligament (LTIL).
.Distal row
- trapeziotrapezoid ligament
- trapeziocapitate ligament
- capitohamate ligament
.Palmar midcarpal
- scaphocapitate (SC)
- triquetral –hamate-capitate (THC)")
: Coronal and axial DP FS showing its dorsal (dSLIL) and volar portion (pSLIL).")
: Coronal DP FS and T1WI and axial DP FS showing its dorsal (dLTIL) and palmar portion (pLTIL).")
 ligament
On the right, capitohamate (CH) ligament")
 composed by the bones on the proximal row of the carpus (scaphoid, lunate, and triquetram).
These bones have no muscle insertions and their movement is dictated by the surrounding articulations.")

- along the distal aspect of the proximal row of carpal bones (II - purple)
- along the proximal convex curvature of the capitate and hamate (III - blue)
Disruption of these arcs, or any overlapping of adjacent bones, commonly indicates underlying carpal instability or fracture.")
.")
: intersection of a line drawn parallel to the long axis of the scaphoid and a line drawn perpendicular to the AP axis of the lunate. Normal range between 30-60º.
- Capitolunate angle (right): intersection of a line drawn parallel to the long axis of the capitate and a line drawn perpendicular to the AP axis of the lunate. It should measure less than 30º in resting position.")
 and stress radiographs are normal.
Axial fat-satturated DP demonstrate a disruption of the scapholunate ligament (blue arrows), with surrounding soft tissue oedema.")
 but the instability becomes evident in stress view such as clenched fist or radial–ulnar deviation views (PA clenched fist view - right)")
, suspicious for DISI.")
 increased over 70°. This is the most evident sign of SLD.
- Capitolunate angle (right - blue) greater than 15 degrees")

")




 Ilustrated, purely ligamentous axial radial and ulnar dislocations.
(A) Peritrapezoid and peritrapezium axial radial dislocation. With axial radial dislocation, the distal carpus splits longitudinally into two columns: the ulnar column (light blue) is stable with regard to the radius, and the radial column(dark blue) displaces most commonly in the radial and proximal direction.
X-ray sowing a tras-trapezium axial radial dislocation.
(B) Perihamate peripisiform axial ulnar dislocation. In ulnar disruptions, the radial column (light blue) is stable with regard to the radius, and the ulnar column (dark blue) displaces most commonly in the ulnar and proximal direction.")
 Ulnar translocation of the wrist (Taleisnik’s type I). X-ray sohws a widened radioscaphoid joint as well as decreased radiolunate contact length.
(B) Radial translocation of the wrist as a sequel of a malunited distal radius fracture. The ulnar inclination of the radius is pathologically reduced, and the radiolunate contact diameter is increased.")
.")

Right- increased capitolunate angle (normal 0-15 degress)")
 may be seen asociated to the dislocation.")

")

, secondary to malunited fracture on the distal radius.")
, secondary to non-united scaphoid fracture.")