This poster is published under an
open license. Please read the
disclaimer for further details.
Keywords:
Computer applications, Liver, Interventional vascular, MR-Functional imaging, Image manipulation / Reconstruction, Segmentation, Radioembolisation, Computer Applications-General, Cancer
Authors:
S. Thoduka1, P. Schilling1, G. Chlebus2, A. Schenk2, N. Abolmaali1; 1Dresden/DE, 2Bremen/DE
DOI:
10.1594/ecr2017/C-2917
Aims and objectives
Selective internal radiation therapy (SIRT) is a minimally invasive procedure in the treatment of malignant,
non-operable hepatic tumours using microspheres loaded with 90-yttrium delivered directly into tumour-feeding hepatic arteries by an interventional radiologist [1].
As the use of SIRT in the treatment of primary as well as secondary liver tumours increases,
there is an increased need to standardise and optimise the therapy in order to make it more efficient.
The main objective in SIRT is to apply a curative,
targeted dose to the tumour while sparing healthy liver tissue [2].
This requires careful planning of the delivery position through a diagnostic angiographic procedure as well as an accurate calculation of dosage.
Several models for determining dosage have been suggested,
with the more accurate,
modern algorithms primarily dependent on liver and tumour volume measurements [2].
Calculating liver volume and tumour volume in each patient is also an essential step in setting the indication for the therapy [3].
The segmentation of the liver and tumour is a time-consuming task performed by experts.
Our study examines the variability in volumetry performed by an expert compared to that by a novice radiology resident.
Classically,
liver volumetry is performed either using CT or MRI images [4].
In our study we used Gd-EOB-DTPA-enhanced late phase MRI scans,
since these images provide an ideal contrast between the liver and the surrounding organs as well as a high contrast between the liver and metastases,
allowing accurate segmentation of the liver [5] and identification of tumours.
T2w imaging served to exclude benign differential diagnoses,
i.e cysts and hemangiomas.
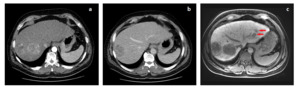
Fig. 1: Comparison of multifocal lesions of hepatocellular carcinoma (HCC) in contrast-enhanced CT in arterial phase (a), in the venous phase (b) and (c) Gd-EOB-DTPA enhanced MRI in the hepatobiliary phase. HCCs reveal different imaging features dependent on their histologic grading: two large lesions in the right liver lobe. MRI using liver specific contrast agent delivers the highest sensitivity: two small lesions in the left liver lobe (arrows). Differences in the pathophysiology of the tumours and the contrast capabilities of imaging techniques may result in differences in volumetry of lesions.
The purpose of our study was to compare volumetric measurements performed by an expert versus a novice radiologist on Gd-EOB-DTPA enhanced liver MRI scans acquired in the hepatobiliary phase using interactive contouring software in planning dosage for SIRT.

 in contrast-enhanced CT in arterial phase (a), in the venous phase (b) and (c) Gd-EOB-DTPA enhanced MRI in the hepatobiliary phase. HCCs reveal different imaging features dependent on their histologic grading: two large lesions in the right liver lobe. MRI using liver specific contrast agent delivers the highest sensitivity: two small lesions in the left liver lobe (arrows). Differences in the pathophysiology of the tumours and the contrast capabilities of imaging techniques may result in differences in volumetry of lesions.")