Renal Lymphangiomatosis is a developmental malformation of normal lymphatic tissue in perirenal or peripelvic area resulting in cystic masses.
Synonyms for this pathology are renal lymphangioma,
hygroma renalis,
and renal lymphangiectasia.
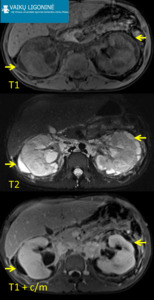
Fig. 1: 14 yo boy was admitted to the emergency department with bilateral flank abdominal pain. Cystic structures around kidneys were reported on US examination. MRI: Pericortical renal cystic lesions(arrows) with fluid signal intensity (T2-WI sequences - high intensity signal, T1-WI sequences with fat saturation with and without contrast material - low intensity signal). Fine needle aspiration revealed lymphatic fluid. Improvement after intramuscular analgesic injection.
References: Department of Radiology, Children‘s Hospital, Affiliate of Vilnius University Hospital Santariskiu Klinikos/ Lithuania 2017
- Best diagnostic clue: Multilocular cystic mass in perirenal area with thin septa.
- Location: Perirenal,
peripelvic; usually bilateral.
- Size: Variable,
can become larger than kidney itself.
- Best imaging tool: MR or CT
- Findings: Subcapsular mass with fluid attenuation on CT and high signal intensity on T2WI MR.
Usually low signal intensity on T1 WI (high signal intensity on T1WI is seen when there is a high proteinaceous material in cyst).
Peripheral and septal enhancement could be found.
Calcification may be seen.
Cystic mass displaces renal parenchyma and adjacent structures.
- Top Differential Diagnoses: Complex fluid collections with enhancing septa (renal and perirenal abscess,
urinoma,
perinephric hematoma),
cystic renal cell carcinoma,
perinephric lymphoma.
- Clinical symptoms: Hypertension,
obstructive uropathy,
dull flank pain,
palpable mass,
hematuria.
- Demographics: Seen in any age.
- Treatment: Conservative management in asymptomatic cases,
percutaneous drainage,
injection of sclerosing agents,
resection of mass.
BPH in young age. Benign prostatic hyperplasia (BPH) is extremely rare in childhood.
In the literature to date five cases have been reported under 18 years of age.
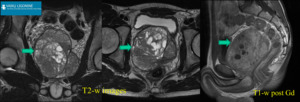
Fig. 2: 16 yo boy was admitted to the emergency department due to urinary retention. US revealed 200 cc pelvic mass. MRI: prostate mass (arrows) with heterogenic signal intensity on T2-WI sequences, without prominent enhancement after contrast media administration. Foley catheter was inserted to relief symptoms. BPH was confirmed after transrectal biopsy. Transvesical enucleation of tumor was performed.
References: Department of Radiology, Children‘s Hospital, Affiliate of Vilnius University Hospital Santariskiu Klinikos/ Lithuania 2017
- Best diagnostic clue: Big mass arising from the prostate,
no enlarged lymph nodes or any sign of metastasis.
- Location: Prostate central zone.
- Size: Variable,
can reach up to 200 cc volume.
- Best imaging tool: MR or US
- Findings: Mass arising from the prostate with radiological characteristics of BPH.
- Top Differential Diagnoses: Sarcoma in prostate.
- Clinical symptoms: Dull pelvic pain,
urinary retention,
urethral discharge without sexual transmitted disease.
- Demographics: Very rare.
- Treatment: Due to the limited number of cases,
the management of BPH in adolescents is unclear.
The endoscopic or open enucleation of lesion is the treatment of choice depending on the experience of surgeon with large volume BPH.
Late complications after surgery of hypospadias. Hypospadias represents one of the most challenging problems in pediatric urology.
The goal of the initial repair is to ensure that the meatus is as distal as possible in order to create a forwardly directed urinary stream.
Failed hypospadias repair manifests early with hypospadias recurrence with an ectopic meatus,
urethral fistula,
urethral stricture,
and ventral penile curvature,
while late complications are strictures,
hair in the urethra,
urethral stones due to hair-bearing skin graft surgery.
The rate of late complications of hypospadias repair has not been well established.
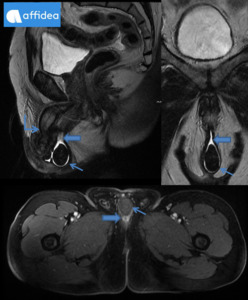
Fig. 3: 14 yo boy with known history of several hypospadia repairs and intermittent dysuria was referred from pediatric urologist to radiology department for MRI exam. MRI: Micropenis (angled arrow) with atypical localisation of an orifice of the urethra. Enlargement of the penile urethra (wide arrows) is seen on T1-WI and T2-WI sequences with intraluminal stones (thin arrows). Buccal mucosa graft surgery was performed.
References: Department of Radiology, Vilnius, Affidea Lietuva/ Lithuania 2017
- Best diagnostic clue: Calcifications in distal deformed urethra.
- Location: Distal urethra.
- Size: Variable,
hairball-stones can become up to 5 cm.
- Best imaging tool: MR,
US
- Findings: Condition is seen after initial correction of hypospadia.
External meatus of the urethra could be not at the top of the glance penis.
Micropenis and lesions in testicles may lead to hypospadia.
Widened urethra proximal to the hairball-stone and bladder wall changes like in sever BPH cases are obtained.
- Top Differential Diagnoses: Urethral stricture.
- Clinical symptoms: Dysuria,
pelvic discomfort,
urinary retention.
- Demographics: Adolescents (hairs grow in skin graft due to puberty and lead to hairball stone formation).
- Treatment: Different options include laser surgery,
grasper extraction,
electrolysis,
and hair tricholysis with thioglycolate.
Buccal mucosa has emerged as the leading graft material in staged repairs to avoid hair in the urethra,
urethral stones.
Herlyn-Werner-Wunderlich (HWW) syndrome is a congenital anomaly of Müllerian ducts and Wolffian structures.
It is known by the triad of didelphys uterus,
obstructed hemivagina and ipsilateral renal agenesis.
Potential acute complications of HWW syndrome are pyohematocolpos,
pyosalpinx,
or pelviperitonitis.
Often and important long-term complications are endometriosis and pelvic adhesions,
that may lead to infertility in maturity.
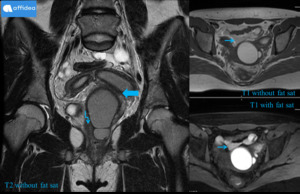
Fig. 4: 13 yo girl referred from district hospital with progressive pelvic pain and dysuria for MRI exam. US examination revealed ovarian cysts and only one kidney. MRI: uterus didelphys, haematometrocolpos, blind-ended distended vagina on the left (wide arrow), normal vagina on the right (angled arrow), blood in uterine tubes and free blood around uterus (thin arrows). HWW syndrome was confirmed. Patient was transferred to the children hospital for immediate colpotomy.
References: Department of Radiology, Vilnius, Affidea Lietuva/ Lithuania 2017
- Best diagnostic clue: Obstructed hemivagina in conjunction with uterus didelphys and ipsilateral renal agenesis.
- Location: Pelvis.
- Size: Size of obstructed hemivagina is variable,
can become very large.
- Best imaging tool: US,
MR
- Findings: Signs of haematocolpos,
haematometrocolpos,
fluid or blood in adnexal region and pelvis,
didelphys uterus along with ipsilateral renal agenesis,
or other Wolffian structures anomalies such as duplicated kidneys,
or dysplastic kidneys,
or crossed fused ectopia are present.
Endometriotic cysts may be present in ovaries,
which appear hyperintense on T1-WI and mildly hypointense or hyperintense on T2-WI on MRI studies.
- Top Differential Diagnoses: Large pelvic mass that could lead to vaginal obstruction,
other Müllerian ducts anomalies.
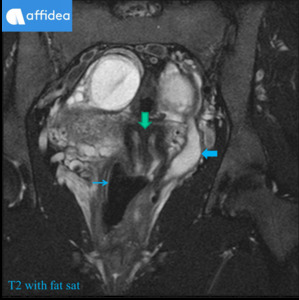
Fig. 5: 16 yo girl referred by urologist for MRI exam due to dull intermittent pelvic pain. US examination showed only one kidney, ovarian cysts and uterus didelphys. MRI: uterus didelphys(vertical arrow), one normal vagina (thin arrow), cystic elongated structure with an opening to the vagina (wide arrow). Elongated structure is thought to be a remnant of undeveloped Müllerian ducts. Conservative treatment was applied.
References: Department of Radiology, Vilnius, Affidea Lietuva/ Lithuania 2017
- Clinical symptoms: Pelvic pain after menarche,
increasing pelvic pain during periods,
dysmenorrhea and palpable pelvic or perineal mass due to the associated haematocolpos or hematometra,
which result from retained menstrual flow.
- Demographics: At puberty - due to menstrual blood collections in the obstructed hemivagina.
- Treatment: Surgical puncture of obstructed hemivagina to relieve the obstruction.
Endometriosis surgery and reconstructions surgery at the second stage.
Persistent urethral diverticulum in female is a focal outpouching of the urethra.
Synonym for this pathology is urethrocele.
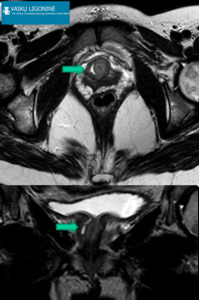
Fig. 6: 12 yo girl referred by urologist for MRI investigation due to unexplained prolonged dysuria. US examination does not revealed any abnormalities. MRI: additional cystic structure (arrows) around distal urethra from the right side (high intensity signal on T2-WI) with a canal and an opening to the urethra lumen. Persistent urethral diverticulum was removed surgically.
References: Department of Radiology, Children‘s Hospital, Affiliate of Vilnius University Hospital Santariskiu Klinikos/ Lithuania 2017
- Best diagnostic clue: Unilocular or multilocular cystic lesion that communicates with the posterolateral mid or distal urethral lumen.
It often wraps around the urethra.
- Location: Mid urethra.
- Size: Variable,
can become up to 5 cm.
- Best imaging tool: US,
MR
- Findings: Anechoic unilocular or multiple cystic structure is seen on transvaginal,
transperineal or transabdominal US investigation.
Diverticulum is T1WI hypointense on MRI.
T2WI shows the presence of hyperintense fluid in a diverticulum.
T1WI after contrast material administration is useful for detection of inflammation or infection.
- Top Differential Diagnoses: Skene`s duct cyst,
vaginal wall cyst,
ectopic ureterocele.
- Clinical symptoms: Dysuria,
dribbling and urinary retention in female.
- Demographics: Occur more usually in women between the 3rd and 5th decades of life but can affect all age groups.
- Treatment: Surgical removal is the mainstream of treatment for urethral diverticula.
Vaginal atresia is a congenital defect resulting in uterovaginal outflow tract obstruction.
It occurs from a failure of recanalisation of the urogenital sinus.

Fig. 7: 4 yo girl was admitted to the emergency department due to pelvic/perineal pain and dysuria. Vaginal atresia or stenosis was suspected on physical examination. Transabdominal US exam does not reveal any abnormalities. MRI: cystic structure (wide arrows, high signal on T2-WI, low signal on T1-WI sequences) located behind distal urethra (thin arrow). Vaginal atresia was confirmed, colpotomy was performed.
References: Department of Radiology, Children‘s Hospital, Affiliate of Vilnius University Hospital Santariskiu Klinikos/ Lithuania 2017
- Best diagnostic clue: Obstructed vagina.
- Location: Superior,
mid- or inferior vagina.
- Size: Variable,
can become very large.
- Best imaging tool: MR or US
- Findings: The diagnosis may be suggested in utero when performing ultrasound if there is obstruction causing significant amount of hydrocolpos or mucocolpos.
Depending on the site of atresia and state of menstruation there can be a combination of hydrocolpos,
hydrometra,
hydrometrocolpos,
haemetocolpos,
haemetometrocolpos,
haemetometra.
At MR imaging,
the vaginal wall anatomy is best depicted with T2-weighted sequences.
- Top Differential Diagnoses: Vaginal stenosis,
transverse vaginal septum,
congenital uterovaginal anomalies including HWW syndrome,
imperforate hymen.
- Clinical symptoms: Primary amenorrhoea and cyclic pelvic pain.
- Demographics: Mostly at puberty due to menstruation blood collections in the obstructed vagina or in neonates due to collection of mucous.
- Treatment: vaginal repair surgery.

 with fluid signal intensity (T2-WI sequences - high intensity signal, T1-WI sequences with fat saturation with and without contrast material - low intensity signal). Fine needle aspiration revealed lymphatic fluid. Improvement after intramuscular analgesic injection. References: Department of Radiology, Children‘s Hospital, Affiliate of Vilnius University Hospital Santariskiu Klinikos/ Lithuania 2017")
 with heterogenic signal intensity on T2-WI sequences, without prominent enhancement after contrast media administration. Foley catheter was inserted to relief symptoms. BPH was confirmed after transrectal biopsy. Transvesical enucleation of tumor was performed. References: Department of Radiology, Children‘s Hospital, Affiliate of Vilnius University Hospital Santariskiu Klinikos/ Lithuania 2017")
 with atypical localisation of an orifice of the urethra. Enlargement of the penile urethra (wide arrows) is seen on T1-WI and T2-WI sequences with intraluminal stones (thin arrows). Buccal mucosa graft surgery was performed. References: Department of Radiology, Vilnius, Affidea Lietuva/ Lithuania 2017")
, normal vagina on the right (angled arrow), blood in uterine tubes and free blood around uterus (thin arrows). HWW syndrome was confirmed. Patient was transferred to the children hospital for immediate colpotomy. References: Department of Radiology, Vilnius, Affidea Lietuva/ Lithuania 2017")
, one normal vagina (thin arrow), cystic elongated structure with an opening to the vagina (wide arrow). Elongated structure is thought to be a remnant of undeveloped Müllerian ducts. Conservative treatment was applied. References: Department of Radiology, Vilnius, Affidea Lietuva/ Lithuania 2017")
 located behind distal urethra (thin arrow). Vaginal atresia was confirmed, colpotomy was performed. References: Department of Radiology, Children‘s Hospital, Affiliate of Vilnius University Hospital Santariskiu Klinikos/ Lithuania 2017")
 around distal urethra from the right side (high intensity signal on T2-WI) with a canal and an opening to the urethra lumen. Persistent urethral diverticulum was removed surgically. References: Department of Radiology, Children‘s Hospital, Affiliate of Vilnius University Hospital Santariskiu Klinikos/ Lithuania 2017")