For this prospective study we conducted a randomized sampling of morbidly obese patients which had undergone bariatric surgery three years before,
obtaining 40 patients.
The inclusion criteria were:
- To fulfil the Spanish Society for the Study of Obesity (SEEDO) criteria concerning the indication of bariatric surgery
- To have a preoperative clinical-radiological assessment including blood tests,
ultrasound examination and determination of shear wave velocity of the liver with acoustic radiation force impulse (ARFI)
- To undergone a intraoperative biopsy which showed features consistent with NAFLD
The exclusion criteria were:
- Administration of medication that might have adverse affects on the liver
- Human immunodeficiency virus infection
- Viral hepatitis
- Alpha-1-antitrypsin deficit
- Metal deposition diseases
- Alcohol consumption of greater than 20 g/day
The study was approved by the local ethics committee.
All patients provided written informed consent.
Clinical-radiological assessment
1- Clinical examination
All patients were measured and weighed,
barefoot and in light clothing,
to determine their body max index (BMI).
2- Laboratory tests
Venous blood samples were obtained after a 12-h overnight fast and total cholesterol,
low-density lipoproteins,
triglycerides,
glutamate oxaloacetate transaminase,
glutamate pyruvate transaminase and platelets were measured.
3- Radiologic assessment
The patients were evaluated the day before surgery.
An ACUSON 2000 platform 2000 (Siemens,
Erlangen,
Germany),
equipped with a 4–1 MHz multi-frequency convex probe was used.
The examination was conducted by a radiologist with more than 23 years’ experience in abdominal ultrasound and 3 years’ experience in elastography who was blinded to the other study results.
Patients did not fast beforehand.
The technique was performed with the patient supine,
the right arm in maximum abduction and the probe over the skin in the intercostal space between the 9th and 10th ribs with breath-holding.B-mode images were obtained of the right liver lobe and the region of interest (ROI) was positioned in segment VI at a depth of 3.5–8 cm below the hepatic capsule,
which means we had no problems in performing ARFI in patients with morbid obesity.
Fig. 5
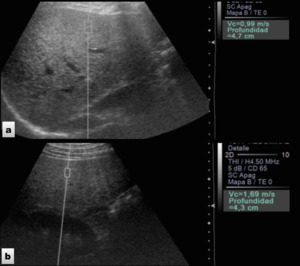
Fig. 5: ARFI technique. a) Healthy volunteer who underwent liver elastography which demonstrated normal SWV (0.99m/s). b) Patient with NAFLD who showed increased liver SWV (1.69m/s).
The definitive shear wave velocity (SWV) was obtained from the mean of the three SWVs taken successfully.
The number of attempts to obtain correct measurements was 4±1 (range 3–8).
The measure was considered incorrect by motion artefact when it was “xxx”.
Before ARFI a conventional hepatic ultrasound study was conducted by the same radiologist to determine the subjective grade of steatosis observed (none,
mild,
moderate and severe).
Steatosis was subjectively classified according to the increase in echogenicity of the hepatic parenchyma in comparison to the cortical echogenicity of the right kidney and the decrease in visualisation of the diaphragm and hepatic vessels. Fig. 6
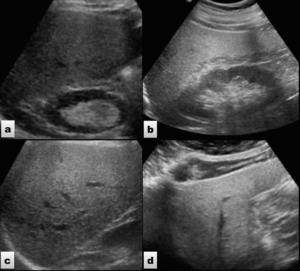
Fig. 6: Ultrasound images showing different grades of liver steatosis. a) Mild steatosis. b and c) Moderate steatosis. d) Severe steatosis
Statistical analysis
The statistical analysis was conducted with the SPSS statistical software package version 15.0 (SPSS forWindows,
Chicago,
IL,
USA).
Qualitative variables were described with absolute and relative frequencies.
The results of quantitative variables were expressed as mean ± standard deviation (range).
The distribution of the variables was analysed using the Kolmogorov–Smirnov test.
The quantitative variables with a normal distribution were analysed using Student’s t test.
Student’s t test was used to compare the means between the SWVs before and after surgery. The chi-squared (χ2) test was used to compare qualitative variables before and after surgery.
Differences were considered statistically significant at P<0.05.

 Healthy volunteer who underwent liver elastography which demonstrated normal SWV (0.99m/s). b) Patient with NAFLD who showed increased liver SWV (1.69m/s).")
 Mild steatosis. b and c) Moderate steatosis. d) Severe steatosis")