Now that we have reviewed the key concepts about cholangiopathies,
we can exemplify them dividing into: genetic,
immune-mediated,
idiopathic,
infectious,
vascular and obstructive.
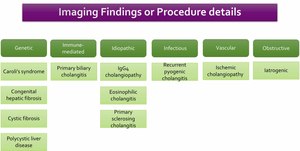
Table 1
Genetic
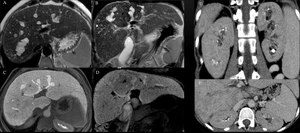
Fig. 1: A-D: Multifocal cystic dilatation of segmental intrahepatic bile ducts. Gadoxetic acid enhanced-MRI shows contrast excretion into dilatated intrahepatic bile ducts. E-F: CECT shows medullary sponge kidney, a sporadic condition associated with Caroli Disease.
Definition: Caroli disease,
or communicating ectasia of the intrahepatic bile ducts,
is a rare and autosomal recessive disorder that is part of the clinicopathologic spectrum of ductal plate malformations.
If the large intrahepatic bile ducts are affected,
the result is Caroli disease,
whereas abnormal development of the small intrahepatic bile ducts results in congenital hepatic fibrosis.
If all levels of biliary tree are involved,
features of both congenital hepatic fibrosis and Caroli's disease are present being named "Caroli's syndrome.”
Clinical presentation: related to biliary stasis,
such as abdominal pain,
fever.
The occurrence of Caroli disease alone is uncommon; The Caroli syndrome occurs more frequently.
This disease is also associated with the occurrence of medullary sponge kidney,
autosomal dominant polycystic kidney disease and autosomal recessive polycystic kidney disease.
Image key points: duct dilatation,
fibrosis,
and inflammation result in a wide spectrum of radiologic features.
The disease may present saccular or fusiform biliary dilatation.
Fibrovascular bundles within or along the edge of the dilated ducts have been termed the central-dot sign.
The cholangiographyc features of Caroli disease include saccular dilatation,
irregular bile duct walls,
strictures,
and stones.
The diagnostic challenge with MR is accurate identification of communicating cystic biliary dilatation.
- Congenital hepatic fibrosis
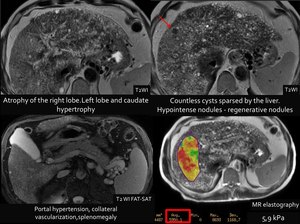
Fig. 2
References: Fleury Medicina Diagnóstica, São Paulo, Brazil
Case: Report: Estimated liver fat fraction: 7% (normal up to 5%).Hepatic rigidity estimated by elastography: 6.2 kPa (indicative of F4 fibrosis).
Definition: is a developmental malformation that belongs to the family of hepatic ductal plate malformation.
CHF is a congenital multisystemic disorder,
mostly inherited in autosomal recessive fashion.
Main underlying process of the disease is the malformation of the ductal plate.
It is almost always associated with autosomal recessive polycystic kidney disease.
Clinical presentation: nonspecific.
The most common manifestations are those related to portal hypertension.
Image key points: Liver - Morphological alterations of the liver: hypertrophy of the left lateral segment and caudate lobe,
normal or hypertrophic left medial segment,
atrophic right lobe.
An enlarged hepatic artery with associated large regenerative nodules as a consequence of augmented arterialization of the liver.
Ductal dilations can be seen in all imaging modalities and continuous and non-continuous tubular cystic structures and fibrosis can be seen periportal thickening.
Kidneys -Parenchymal cysts.
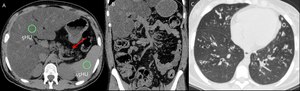
Fig. 3: A-C: non enhanced CT. A 20-year-old female with cystic fibrosis. A- mean hepatic attenuation:5HU and fatty replacement in of pancreatic parenchyma (arrow). C- Pulmonary bronchiectasis
Definition: autosomal recessive genetic disease that affects the exocrine function of the lungs, liver, pancreas and small bowel,
caused by mutations in the CF transmembrane conductance regulator (CFTR) gene.
Epidemiology: It is the most common autosomal recessive genetic disease in white people,
affecting 1 in 3000 births in the United States.
Clinical presentation: It has a varied clinical presentation: neonatal cholestasis to asymptomatic elevation of liver transaminases,
liver steatosis,
focal biliary cirrhosis,
and liver cirrhosis with or without portal hypertension.
The most common presentation of liver disease in patients with CF is hepatomegaly.
Image key points: Hepatic manifestations range from hepatomegaly and diffuse fatty infiltration to severe cirrhosis with fibrotic change,
regenerative nodules,
and portal hypertension.
Splenomegaly is also common.
Pancreas: fat deposition,
pancreatic cysts and duct abnormalities are also occasionally seen.
Biliary: cholelithiasis,
stricturization,
and narrowing or dilatation of intra- and extrahepatic bile ducts.
Gallbladder: microgallbladder are also readily demonstrated.
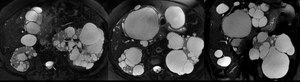
Fig. 4: A 70-year-old woman with polycystic kidney disease. A-B: Axial T2WI FAT-SAT; C Coronal T2WI FAT-SAT: cysts of varying size diffusely distributed in the liver and kidneys.
Definition: Polycystic liver disease (PLD) is a hereditary condition that may arise either in patients with autosomal dominant polycystic kidney disease (ADPKD) or in patients with a different genetic mutation that results in autosomal dominant polycystic liver disease.
It is characterized by progressive development of hepatic cysts.
Clinical presentation: Asymptomatic in most cases.
Symptomatic patients have massive hepatomegaly.
Image key points: Two types of cysts may be found in the liver: intrahepatic cysts and peri-biliary cysts.
It is important to look for signs of complication of the cysts,
which can be suggested by increased T1WI MRI,
heterogeneous echotexture at US,
or increased attenuation at unenhanced CT (which may suggest a hemorrhagic cyst).
Other signs of complication associated with infection are fluid-fluid level in the cyst,
cyst wall thickening or calcification,
and intracystic gas bubbles.
Immune-mediated
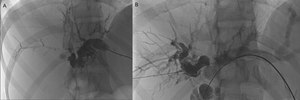
Fig. 5: A 37-year-old woman presented with abdominal pain and cholestatic syndrome for 3 months.
A-B (Percutaneous transhepatic cholangiography) - in A, left hepatic duct catheterization; in B, catheterization of the right hepatic duct. In both, dilatation of the intrahepatic biliary tract with "beaded appearance" and ductal stenosis at the level of the confluence of the right and left hepatic ducts is demonstrated.
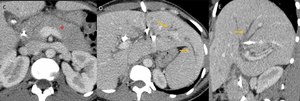
Fig. 6: Same case as Fig.5:
C-D (Axial CT venous phase) and E (Sagital CT venous phase) - after percutaneous drainage biliary tree - in C, pancreas has signs of autoimmune pancreatitis, enlargement of the pancreas with loss of definition of the pancreatic clefts (*); in D and E, irregular dilations of the biliary tree (arrows).
Definition: IgG4 cholangiopathy is considered one of the systemic diseases related to IgG4.
After the pancreas,
the bile ducts are the second most common site of involvement.
This disease is considered as one of the secondary causes of sclerosing cholangitis.
Epidemiology:: It occurs more in men,
around the age of 60.
Clinical presentation: Painless obstructive jaundice frequently accompanied by autoimmune pancreatitis.
Radiographic features: Involvement of the intrapancreatic distal common bile duct and hilar bile duct; late circumferential enhancement of biliary ducts involved; segmental and circumferential parietal thickening,
with visible lumen; findings of autoimmune pancreatitis and extra-biliary findings associated with IgG4 disease; long and continuous stenosis of bile ducts with pre-stenotic dilatation.
Image key points: Stenosis hilar bile duct (hepatic confluence) associated with CT signals pancreatic disease involvement.
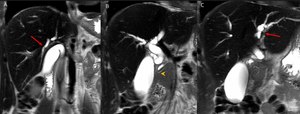
Fig. 7: A 36-year-old man presented with abdominal pain, jaundice, pruritus and serum eosinophilia and had a history of eosinophilic pneumonia. Coronal T2WI-MRI (A-C):dilatation of the intrahepatic and extrahepatic bile ducts (→). In B, the common bile duct is narrowed in its intrapancreatic portion (arrowhead)
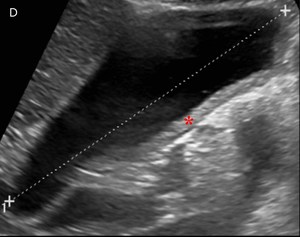
Fig. 8: Same case as Fig. 7
D- Ultrasonography demonstrates thickening of the gallbladder wall (*).
Definition: Rare benign disease caused by eosinophilic infiltration of the biliary system.
This disease is considered as one of the secondary causes of sclerosing cholangitis.
Epidemiology: Prevalence in middle-aged men.
Clinical presentation:Jaundice,
abdominal pain (eosinophilic gastroenteritis),
serum eosinophilia (approximately 50%).
Frequently self-limited clinical course,
or regression after corticotherapy
Radiographic features: Thickening of the wall of the gallbladder and extrahepatic bile ducts especially of the proximal portion of the common bile duct and cystic duct; diffuse stenosis of the bile ducts in the region of the confluence of the right and left hepatic ducts and intrahepatic ducts; focal stenosis of the common hepatic duct at the level of cystic duct insertion; discrete narrowing of the proximal commom bile duct.
Image key points: Thickening of the gallbladder wall.
- Primary sclerosing cholangitis
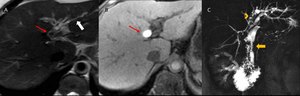
Fig. 9: A 48-year-old woman with Crohn's disease and cholecystectomy presented a transient increase in bilirubin. A (Axial T2): irregular dilatation of intrahepatic bile ducts (white arrow) and hepatolithiasis (red arrows in A and B - Axial non-enhanced T1WIFS).In C (Coronal T2 Gad cholangiographic phase): extensive filling defect is observed in the left hepatic duct (arrowhead) and a narrowing of the proximal common bile duct (yellow arrow).
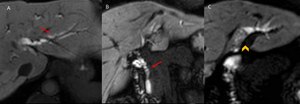
Fig. 10: Same case as Fig. 9
MRI obtained 60 minutes after hepatobiliary-specific contrast media injection. A-B: irregular dilatation of the intrahepatic bile ducts with a “bead appearance”(A) and dilation of the extrahepatic bile ducts (B); In C: there is a filling defect in the left hepatic duct.
Epidemiology: Rare disease,
more prevalent in men (2 men: 1 woman) young.
It is associated with inflammatory bowel disease (IBD) in 60-80% of cases: it is associated with ulcerative colitis (RCU) in 87% and Crohn's disease (CD) in 13%.
Etiology is still unknown,
and is not considered an autoimmune disease.
It is not related to IgG4 disease (in the recent literature,
it is considered a distinct pathology,
classified as a secondary cause).
Radiographic features: It usually involves intra- and extra-hepatic ducts presenting: multifocal stenosis and segmental dilations - being able to form an "bead appearance"; may present with diverticula-like images: in its late onset: filling defects in the biliary tree,
promoting a pruned tree appearance.
Image key points: Involvement of the intra- and extrahepatic biliary tract; “bead appearance”.
Infectious
- Recurrent Pyogenic Cholangitis
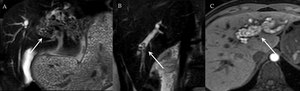
Fig. 11: A 26-year-old female presented with jaundice, pruritus, nausea, vomiting, pain in the right hypochondrium and weight loss of 10 kg in 7 months. Laboratory tests were suggestive of cholestasis and infection.
Coronal T2WI-MRI (A-B) demonstrates intrahepatic bile duct stones as multiple filling defects in the left liver lobe (A) and in the right liver lobe (B). Axial T1WI (C) the intrahepatic stones have high signal intensity (pigment stones)
Definition: Recurrent episodes of biliary sepsis leads to the formation of pigmented biliary stones and,
with the progression,
to the formation of inflammatory stenoses of the biliary tree.
This condition is widely associated with parasites such as those caused by Clonorchis sinensis or Ascaris lumbricoides.
This disease is considered as one of the secondary causes of sclerosing cholangitis.
Epidemiology: It affects people in the 6th and 7th decades of life,
coming from rural areas and with a low socioeconomic level.
It is endemic in Southeast Asia.
Radiographic features: Hepatolithiasis,
with pigmented biliary stones; dilation of the central intrahepatic bile ducts and extrahepatic ducts associated with a decrease decreased arborization,
and abrupt nonvisualization of the peripheral branches.
Vascular
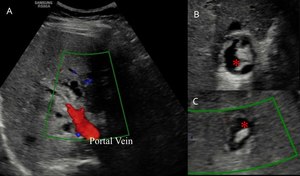
Fig. 12: A 37-year-old man in late postoperative stage of liver transplantation for fulminant hepatitis of undetermined cause. Doppler ultrasonography (A) showing the hepatic hilum, with the portal vein in red, and the hepatic artery with no detectable flow. B-C: extrabiliary collections of bile, the "bilomas" - (*).

Fig. 13: Same case as Fig. 12: Evolution with cholestatic syndrome and increase of canalicular enzymes. D-E: MR Cholangiography with tapering of the common hepatic duct / common bile duct (arrowhead) and irregular dilatation of the intrahepatic bile ducts with formation of bilomas (arrow). F: Percutaneous trans-hepatic cholangiography - filling defect of the common hepatic duct / common bile duct and a dilated and irregular intrahepatic biliary tree.
Definition: The main mechanism of injury is due to the fact that the bile ducts are vulnerable to ischemia because they essentially depend on the arterial supply.
This disease is considered as one of the secondary causes of sclerosing cholangitis.
Epidemiology: Diagnosis suggested by the history compatible with the possibility of arterial lesion.
Clinical presentation:.
Acute: fever,
abdominal pain,
jaundice,
biliary sepsis; Chronic: Progressive or fluctuating cholestasis is associated.
Radiographic features: Initial stage : Ischemic biliary epithelium peels and forms the "mold" of the biliary tree; Intraductal filler defects and ductal dilation (obstruction caused by epithelium peeling material) - may simulate intrahepatic bile stone; If severe ischemia occurs,
necrosis of the entire ductal wall thickness causes bile overflow in the hepatic parenchyma,
forming bilomas.
Late stage: - Stenosis and dilation (non-specific).
Diagnosis suggested by the history,
arterial lesion in the image and location of the stenoses in the middle third of the common bile duct and the hilar portion of the common hepatic duct.
Image key points: Hepatic artery thrombosis; Biloma; Intra ductal filling faults; Stenosis of the common hepatic duct / bile duct.
Obstructive
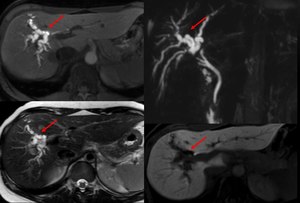
Fig. 14: Patient with obstruction due to iatrogenic lesion of the bile duct after cholecystectomy, presents dilatation of the right hepatic duct and its branches (arrows)
Definition: Secondary cholangiopathy characterized by inflammation,
fibrosis,
destruction of the biliary tree due to obstruction of the biliary tract.
The pathological changes depend on the duration and degree of obstruction and biliary stasis,
as well as the presence of concomitant infection.
This disease is considered as one of the secondary causes of sclerosing cholangitis.
Etiologies: Post-cholecystectomy surgical trauma.
(one of the main obstructive etiologies) or other surgeries; intraductal gallstones; Cholelithiasis or cholecystitis; polyps; neoplasms; pancreatic diseases.
Clinical presentation: Biliary obstruction can cause biliary stasis and / or cholangitis.
Radiographic features: Gallstones; dilatation of the bile ducts; hepatic abscess (late stage)
Practical Guide – Cholangiopathies
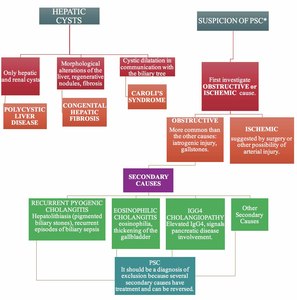
Table 2: Practical Guide -
PSC: Primary Sclerosing Cholangitis:
*bead appearance of the biliary tree, strictures, segmental dilatation, pruned tree aspect.




. C- Pulmonary bronchiectasis")

 - in A, left hepatic duct catheterization; in B, catheterization of the right hepatic duct. In both, dilatation of the intrahepatic biliary tract with "beaded appearance" and ductal stenosis at the level of the confluence of the right and left hepatic ducts is demonstrated.")
 and E (Sagital CT venous phase) - after percutaneous drainage biliary tree - in C, pancreas has signs of autoimmune pancreatitis, enlargement of the pancreas with loss of definition of the pancreatic clefts (*); in D and E, irregular dilations of the biliary tree (arrows).")
:dilatation of the intrahepatic and extrahepatic bile ducts (→). In B, the common bile duct is narrowed in its intrapancreatic portion (arrowhead)")
.")
: irregular dilatation of intrahepatic bile ducts (white arrow) and hepatolithiasis (red arrows in A and B - Axial non-enhanced T1WIFS).In C (Coronal T2 Gad cholangiographic phase): extensive filling defect is observed in the left hepatic duct (arrowhead) and a narrowing of the proximal common bile duct (yellow arrow).")
 and dilation of the extrahepatic bile ducts (B); In C: there is a filling defect in the left hepatic duct.")
 demonstrates intrahepatic bile duct stones as multiple filling defects in the left liver lobe (A) and in the right liver lobe (B). Axial T1WI (C) the intrahepatic stones have high signal intensity (pigment stones)")
 showing the hepatic hilum, with the portal vein in red, and the hepatic artery with no detectable flow. B-C: extrabiliary collections of bile, the "bilomas" - (*).")
 and irregular dilatation of the intrahepatic bile ducts with formation of bilomas (arrow). F: Percutaneous trans-hepatic cholangiography - filling defect of the common hepatic duct / common bile duct and a dilated and irregular intrahepatic biliary tree.")
")
