Opportunistic infections:
Toxoplasmosis:
CT findings: Multiple areas of low attenuation in the basal ganglia,
thalamus and corticomedullary junction.
May be hyperdense if hemorrhagic.
After administration of IV contrast material these areas demonstrate ring or nodular enhancement (patients with decimated immune systems may not show enhancement).
After treatment,
calcifications may be evident.
MRI findings: On T2-weighted sequences,
lesions appear hypo- to isointense with surrounding high signal intensity vasogenic edema.
On postcontrast MRI there is evidence of multiple nodular lesions or ring enhancing lesions some with an eccentric nodule the so called “target sign”. Hemorrhage may be observed in some cases.
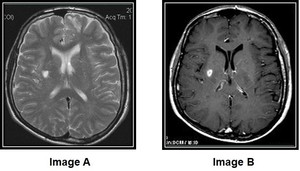
Fig. 1: Cerebral toxoplasmosis
Image A: MR T2 weighted image illustrates a hyper-intense lesion located in the right basal ganglia with faint regional edema.
Image B: MR T1 weighted sequence after gadolinium administration demonstrates in the same location a peripherally enhancing nodule.
References: References: 2nd department of Radiology, University hospital of Athens " ATTIKON" - Athens/GR
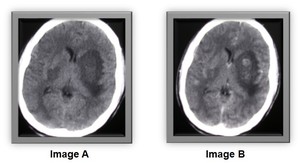
Fig. 2: Cerebral toxoplasmosis
Image A: Axial plane of a pre - contrast CT image/ Presence of a few hypodense regions in the basal ganglia more evident on the left side where mass effect is observed on the frontal horn of the ipsilateral lateral ventricle with concomitant effacement of the adjacent sulci.
Image B: Axial plane of a post - contrast CT image demonstrates in the same locations a few peripherally enhancing nodules.
References: References: 2nd department of Radiology, University hospital of Athens " ATTIKON" - Athens/GR
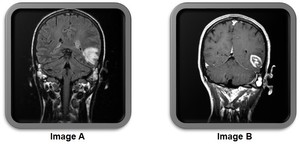
Fig. 3: Cerebral toxoplasmosis Image A: MR FLAIR image illustrates a hypo-intense lesion located in the left temporal lobe with regional hyper-intense area – edema and effacement of nearby sulci.Image B: MR T1 weighted sequence post – gadolinium evidences the lesion with ring enhancement and centrically located enhancing nodules.
References: References: 2nd department of Radiology, University hospital of Athens " ATTIKON" - Athens/GR
CMV:
CT and MRI imaging may be normal.
On the other hand signs of demyelination can be evident as areas of low attenuation in the white matter on CT which correspond to hyperintense areas on T2 weighted MR images.
Moreover CNS involvement can appear as ependymitis,
meningoencephalitis or ventriculitis.
On CT images low attenuation is present in the white matter with ependymal enhancement on post contrast CT images.
On T2-weighted MR images there is focal or diffuse hyperintensity in the white matter accompanied by ependymal,
subependymal and periventricular T2 increased signal.
Furthermore there is ependymal enhancement on post contrast T1 weighted sequences in ventriculitis.
There is no evidence of mass effect and hydrocephalus may be seen.
TB:
1) Signs of meningitis,
more noticeable in the basilar cisterns.
2) Hydrocephalus,
3) Abscesses which demonstrate ring enhancement 4) Tuberculomas: Tend to be smaller than abscesses,
may be solitary or multiple,
usually supratentorial,
can also appear in subdural,
epidural and subarachnoid spaces.
In early stages they are hypointense on T2-weighted MR images and in later phases they develop a hypointense center surrounded by an iso-intense capsule and may further progress to abscesses with a hyper-intense center.
5) Ischemia and infarction due to vasospasm and thrombosis of the arteries that supply the basal ganglia are uncommon findings.
Fungal:
Cryptococcal infection: Most common location: basal ganglia,
thalamus and cerebellum.
Imaging features include: meningoencephalitis,
hydrocephalus,
gelatinous pseudocysts resulting in dilated perivascular spaces and cryptococccomas in a intraventricular or intraparenchymal location.
CT findings: Can present with normal scans,
or signs of diffuse atrophy,
hydrocephalus and mass lesions.
MRI Findings: Meningeal disease demonstrates leptomeningeal enhancement on post-gadolinium T1-weighted images and cryptococcomas appear with low signal on T1-weighted images,
high signal on T2 and varying enhancement patterns on T1 after gadolinium administration,
ranging from no enhancement to peripheral nodular enhancement.
Finally gelatinous pseudocysts show low to intermediate (from mucin) signal on T1,
high signal on T2 and low on FLAIR.
Dilated perivascular spaces more evident on MR images.
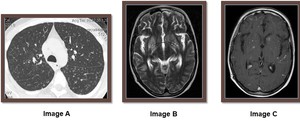
Fig. 4: Cryptococcal infection Image A: Axial CT image in lung window setting illustrates numerous, bilateral, smaller than 10mm nodules scattered throughout the upper lobes and superior segments of the lower lobes. Image B: Same patient/ MRI T2 weighted sequence reveals dilated perivascular spaces / Virchow-Robin spaces in bilateral basal ganglia.Image C: MRI T1 weighted sequence post – gadolinium demonstrates scattered foci of enhancement more evident in bilateral basal ganglia as well as meningeal enhancement.
References: References: 2nd department of Radiology, University hospital of Athens " ATTIKON" - Athens/GR
Aspergillosis:
Results from angioinvasive infection of the central nervous system and may cause and present with imaging findings of acute infarction,
infectious cerebritis,
abscess,
hemorrhage and invasive paranasal rhinosinusitis,
acute or chronic,
with osteomyelitis or intracerebral extension which may consist of secondary intracranial dural enhancement and subdural empyema.
However,
it is important to note that aspergillus abscesses may also have peripheral low signal on T2-weighted images which is likely due to surrounding hemorrhage (better seen on GRE or SWI images).
In rare cases aspergillosis may present as a tumour-like mass lesion which appear hypo-to-isointense on T1-weighted images,
hypointense on T2-weighted images,
and demonstrate contrast enhancement on post-gadolinium T1-weighted images.
Neurosyphilis: 1) Mild to moderate cerebral atrophy,
2) Leptomeningeal enhancement,
3) Arteritis,
4) Cortical and subcortical infarctions,
5) White matter lesions-regions of nonspecific T2 hyperintensity in the white matter on MRI,
6) Gummas: uncommon finding,
located peripherally in the cerebral cortex,
on CT imaging they present as peripherally located lesions that are isoattenuating compared to the cortex and on MR images they appear isointense to gray matter on T1-weighted sequences and hyperintense on T2 weighted images.
They also demonstrate enhancement after IVC.
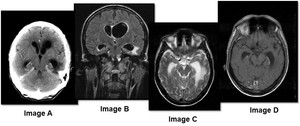
Fig. 5: Neurosyphilis On all images there is brain volume loss with presence of central atrophy-ventriculomegaly. Image A: Axial post contrast CT scan depicts a focal area of hypo attenuating –non enhancing periventricular white matter adjacent to the temporal horn of the left lateral ventricle. Image B: Coronal plane of MRI FLAIR sequence demonstrates an area of high signal intensity in the same position as before. Image C: Axial MRI T2 weighted sequence nicely presents the same finding as a hyper intense appearance of the periventricular white matter. Image D: Axial MRI T1 post – Gadolinium illustrates lack of enhancement
References: References: 2nd department of Radiology, University hospital of Athens " ATTIKON" - Athens/GR
PML:
General findings:
Multiple lesions,
occasionally solitary
Usually no mass effect or hemorrhage.
No vasogenic edema
No enhancement.
Although some cases with faint enhancement have been reported and related with a better survival rate.
Brain volume loss milder then AIDS dementia
Demyelination and necrosis in subcortical white matter.
CT findings: Asymmetric focal zones of low attenuation of the periventricular and subcortical white matter
MRI findings: Asymmetric,
multifocal,
frequently bilateral areas of T1 and T2 prolongation in the periventricular and subcortical white matter.
Subcortical U fibers are frequently involved.
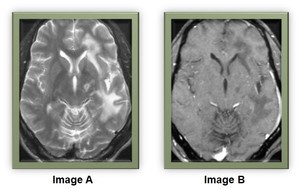
Fig. 6: PML Image A: Axial MRI T2 weighted sequence presents high signal intensity in the periventricular and subcortical white matter (subcortical U-fibers are involved) in the left frontal and temporal lobe with sparing of the cortex. Mild brain volume loss with no mass effect. Image B: Axial MRI T1 image post Gadolinium at the same level demonstrates no evidence of enhancement of the previously mentioned areas.
References: References: 2nd department of Radiology, University hospital of Athens " ATTIKON" - Athens/GR
Bacterial: staphylococcus,
streptococcus: Imaging features of meningitis,
cerebritis,
ventriculitis,
abscesses,
extra-axial collections such as empyema,
thrombosis,
infarct etc.
Directly from HIV itself:
HIV associated neurocognitive disorders (HANDs) - AIDS Dementia Complex:
CT findings:
Atrophic brain compared to patient’s age
Symmetric abnormal low attenuation of the periventricular and deep white matter
No mass effect
No enhancement
MRI findings
Cerebral atrophy
Symmetric,
patchy or confluent areas of T1 and T2 prolongation in the periventricular and deep white matter
No mass effect
No enhancement
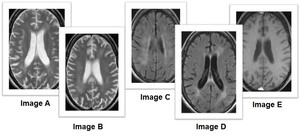
Fig. 7: HIV Encephalitis Image A-B: Axial MRI T2 weighted sequences presents symmetrical high signal intensity in the periventricular white matter, with brain atrophy compared to patients age and no mass effect. Image C-D: Same patient/ MRI FLAIR sequences demonstrate symmetric hyper intensity in the periventricular white matter. Image E: Same patient/ Axial T1 after contrast administration that shows lack of enhancement.
References: References: 2nd department of Radiology, University hospital of Athens " ATTIKON" - Athens/GR
HIV vascular myelopathy:
MRI findings
Volume loss of spinal cord-atrophy (most common finding).
Location: typically the thoracic cord,
but also in some cases the cervical cord.
- Some patients demonstrate bilateral symmetric dorsal column involvement of the spinal cord
CNS Tumors:
Primary CNS Lymphoma (PCNSL): It frequently appears as a solitary mass and less frequently as multiple lesions,
most commonly located in the periventricular white matter,
although it can also originate in the cortex or deep grey matter as well as the corpus callosum.
Typically it is supratentorial and exhibits subependymal spread.
On CT images PCNSL appears iso- to hypo-dense.
On T1 –weighted MR images PCNSL appears hypointense and on T2–weighted MR images iso- to hypo-intense and hyperintense when necrosis exists.
After IVC administration PCNSL usually demonstrates irregular enhancement or ring enhancement in AIDS patients.
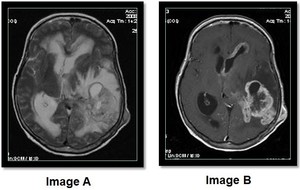
Fig. 8: Lymphoma Image A: MRI Axial T2 weighted sequence illustrates a large heterogeneous mass located in the left temporal lobe, adjacent to the trigone of the left lateral ventricle with hypo-intense and hyper-intense (necrosis) areas. There is also evidence of little mass effect, compared to the size of the lesion, on the left ventricle, mid line shift towards the right side and effacement of the regional sulci. Surrounding increased signal due to vasogenic edema is also observed. There is also increased signal intensity in the periventricular white matter and a heterogeneous mass located on the left side within the soft tissue. Image B: MRI Axial T1 after contrast administration demonstrates irregular enhancement of the same lesion with a central area of non- enhancement due to necrosis and hemorrhage. A similar pattern of enhancement is also evident in the left sided soft tissue mass. Ependymal enhancement of the frontal horn of the left lateral ventricle is also demonstrated.
References: References: 2nd department of Radiology, University hospital of Athens " ATTIKON" - Athens/GR
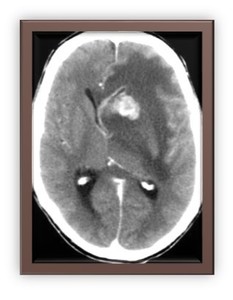
Fig. 9: Lymphoma Axial plane post-contrast CT scan demonstrates a vividly enhancing space occupying lesion in the left basal ganglia with vasogenic edema, midline shift to the right, effacement of the adjacent sulci and compression of the frontal horn of the left lateral ventricle with concomitant ependymal enhancement.
References: References: 2nd department of Radiology, University hospital of Athens " ATTIKON" - Athens/GR
IRIS – Immune reconstitution inflammatory syndrome
The imaging features may demonstrate worsening of the underlying condition.
For example when associated with PML,
new enhancement and mass effect of the previously white matter lesions can be observed.
MRI is the modality of choice when evaluating the CNS in these patients,
but some information can also be obtained from CT scanning.
We present our experience with HIV related CNS pathologies in our department.






 in the left frontal and temporal lobe with sparing of the cortex. Mild brain volume loss with no mass effect. Image B: Axial MRI T1 image post Gadolinium at the same level demonstrates no evidence of enhancement of the previously mentioned areas. References: References: 2nd department of Radiology, University hospital of Athens " ATTIKON" - Athens/GR")

 areas. There is also evidence of little mass effect, compared to the size of the lesion, on the left ventricle, mid line shift towards the right side and effacement of the regional sulci. Surrounding increased signal due to vasogenic edema is also observed. There is also increased signal intensity in the periventricular white matter and a heterogeneous mass located on the left side within the soft tissue. Image B: MRI Axial T1 after contrast administration demonstrates irregular enhancement of the same lesion with a central area of non- enhancement due to necrosis and hemorrhage. A similar pattern of enhancement is also evident in the left sided soft tissue mass. Ependymal enhancement of the frontal horn of the left lateral ventricle is also demonstrated. References: References: 2nd department of Radiology, University hospital of Athens " ATTIKON" - Athens/GR")
