Definition: Herlyn-Werner-Wunderlich (HWW) syndrome,
also known as obstructed hemivagina and ipsilateral renal anomaly (OHVIRA) is a rare form of uterovaginal duplication,
with three characteristic anomalies namely,
didelphys uterus,
unilateral obstructed hemivagina and ipsilateral renal agenesis [1].
It was initially described in 1971 by Herlyn and Werner,
then in 1976,
Wunderlich described an association of right renal aplasia with a bicornuate uterus and simple vagina in the presence of an isolated hematocervix [2].
High index of suspicion of HWW syndrome is required in patients with Mullerian and mesonephric duct anomalies because delay in diagnosis may lead to complications like pelvic adhesions,
endometriosis,
pyocolpos,
pyometra,
and resulting in infertility [3-5].
If this syndrome is suspected,
the diagnosis simply can be made by ultrasound and computed tomography and/or MRI of the abdomen and pelvis [6].
Resection of the vaginal septum is the treatment of choice for obstructive hemivagina [6-7].
Epidemiology: Müllerian duct anomalies have an incidence of 1-5% in the general population and 13-25% in women with recurrent pregnancy loss,
with HWW syndrome constituting 0.16-10% of these anomalies [1].
Overall,
the estimated occurrence of HWW syndrome is 0.1-3.8% [2].
Pathogenesis: HWW syndrome results from an embryologic aberration occurring during the 8th week of gestation that simultaneously involves the metanephric ducts as well as the Paramesonephric or Müllerian ducts.
Failure of complete lateral fusion of the Paramesonephric ducts results in uterus didelphys and lack of development of the metanephric duct results in ipsilateral renal agenesis,
but the exact cause are still unclear [1,8].
The probable causes are polygenic,
multifactorial,
teratogens or environmental [9].
Mehra et al.
explained the embryonic origin of HWW syndrome as the following: embryonic arrest of the caudal portion of one of the Wolffian duct may result from an insult as early as 4th gestation week causes its maldevelopment,
preventing the cross over and subsequent fusion of the Mullerian ducts.
Paramesonephric duct on each side then develops fully with a separate well formed cervix and hemivagina,
resulting in duplication of uteri (uterus didelphys).
Complete nonunion between the paramesonephric ducts and the cranially migrating uterovaginal bulb results in a blind sac or vaginal atresia; while partial non fusion produces a remnant transverse vaginal septum which may be incomplete or complete with obstruction.
Since the ureteric bud develops from the Wolffian duct and ultimately induces the metanephric blastema to form the kidney,
absence of Wolffian duct leads to ipsilateral renal agenesis [1].
Diagnosis and radiologic features: The most frequently used system for classification of Mullerian duct anomalies (MDAs) was proposed by Buttram and Gibbons,
which classifies them into six categories where HWW syndrome is a combination of Type III Mullerian anomaly (uterus didelphys) with mesonephric duct anomaly and vaginal septum [3,10].
But recent study conducted by Zhu et al.based on large population in China,
managed to classify HWW syndrome patients into two new types [2].
Classification 1,
completely obstructed hemivagina
Patients within this classification tend to have an earlier age of onset,
with a short time from menarche to attack (hematocolpos,
hematometra & hematosalpinx).
This is the typical HWW syndrome presentation [11].
The presenting symptoms may include the acute onset of abdominal pain,
fever,
and vomiting.
Also,
patients may progress to secondary endometriosis,
pelvic adhesion,
pyosalpinx,
and even pyocolpos faster if not treated in time [2].
This classification can be further divided into two types:
Classification 1.1,
with blind hemivagina: the hemivagina is completely obstructed therefore the uterus behind the septum is completely isolated from the contralateral uterus.
No communication is present between the duplicated uterus and vagina [2].
Abdominal USG may show absence of kidney with two structures in the pelvis demonstrating the shape,
contour and echo pattern of a uterus.
The endometrial cavity of one of the uterus may be distended with fluid contents and the vagina may not clearly appreciated in continuity with this structure (Fig.
2B).
The other uterus may be of normal size and shape with the myometrium,
endometrial cavity,
cervix as well as vagina (Fig.
2A).
Abdominal MRI may be performed for better characterization of pelvic anatomy.
In sagittal MR images of the pelvis hematometrocolpos may be demonstrated indicating presence of vaginal septum.
T2W coronal or sagittal MR images of pelvis may demonstrate the septum as a hypo intense band in the mid vagina (arrow) (Fig.
3) [1].

Fig. 1: with blind hemivagina
References: Zhu et al. New classification of herlyn-werner-wunderlich syndrome. Chinese medical journal. 2015 Jan 20;128(2):222.
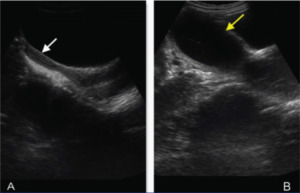
Fig. 2: Ultrasound of pelvis showing two uterine cavities in the pelvis. Right sided uterus with its cervix and vagina (white arrow in A) is normal in size, shape and echo texture with normal endometrial cavity. Left sided uterine cavity (yellow arrow in B) is grossly distended and filled with fluid containing fine internal echoes within.
References: Mehra et al. Imaging Diagnosis of Herlyn-Werner-Wunderlich Syndrome-An Extremely Rare Urogenital Anomaly. Journal of clinical and diagnostic research: JCDR. 2015 May;9(5):TD06.
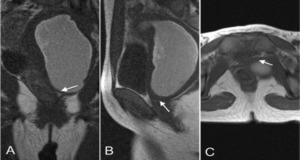
Fig. 3: T2W Coronal, Sagittal MR images of pelvis demonstrating the septum as a hypo intense band in the mid vagina (arrow) causing obstruction and hematometrocolpos.
References: Mehra et al. Imaging Diagnosis of Herlyn-Werner-Wunderlich Syndrome-An Extremely Rare Urogenital Anomaly. Journal of clinical and diagnostic research: JCDR. 2015 May;9(5):TD06.
Classification 1.2,
cervicovaginal atresia without communicating uteri: the hemivagina is completely obstructed; the cervix behind the septum is maldeveloped or atresic,
and menses from the uterus behind the septum cannot outflow through the atresic cervix (Fig.4)[2].

Fig. 4: cervicovaginal atresia without communicating uteri
References: © Zhu et al. New classification of herlyn-werner-wunderlich syndrome. Chinese medical journal. 2015 Jan 20;128(2):222.
Classification 2,
incompletely obstructed hemivagina
These patients have a later age of onset.
The attack often comes years after menarche and usually mild.
Purulent or bloody vaginal discharge can be the chief complaints.
Patients often have ascending genital tract infection.
Complications often develop gradually [2].
This classification also has two sub types:
Classification 2.1,
partial reabsorption of the vaginal septum: a small communication exists between the two vaginas,
which make the vaginal cavity behind the septum incompletely obstructed.
The uterus behind the septum though,
is completely isolated from the contralateral uterus.
The menses can outflow through the small communication,
but the drainage is impeded (Fig.5) [2].

Fig. 5: partial reabsorption of the vaginal septum
References: Zhu et al. New classification of herlyn-werner-wunderlich syndrome. Chinese medical journal. 2015 Jan 20;128(2):222.
Classification 2.2,
with communicating uteri: hemivagina is completely obstructed,
and a small communication exists between the duplicated cervices.
Menses from the uterus behind the septum can outflow through the communication to the offside contralateral cervix.
However because the communication is small,
the drainage is still impeded (Fig.6)[2].

Fig. 6: with communicating uteri
References: Zhu et al. New classification of herlyn-werner-wunderlich syndrome. Chinese medical journal. 2015 Jan 20;128(2):222.
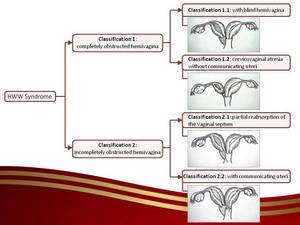
Fig. 7: Classification of HWW syndrome
References: Zhu et al. New classification of herlyn-werner-wunderlich syndrome. Chinese medical journal. 2015 Jan 20;128(2):222.

:222.")
 is normal in size, shape and echo texture with normal endometrial cavity. Left sided uterine cavity (yellow arrow in B) is grossly distended and filled with fluid containing fine internal echoes within. References: Mehra et al. Imaging Diagnosis of Herlyn-Werner-Wunderlich Syndrome-An Extremely Rare Urogenital Anomaly. Journal of clinical and diagnostic research: JCDR. 2015 May;9(5):TD06.")
 causing obstruction and hematometrocolpos. References: Mehra et al. Imaging Diagnosis of Herlyn-Werner-Wunderlich Syndrome-An Extremely Rare Urogenital Anomaly. Journal of clinical and diagnostic research: JCDR. 2015 May;9(5):TD06.")
:222.")
:222.")
:222.")
:222.")