Three patients were identified with HWW syndrome during period of observation from July until December 2016.
The clinical data of these patients was collected from both medical records and history taking.
Radiological features on abdominal CT,
Ultrasonography,
and MRI were demonstrated with simple description.
Abdominal US examination was performed with curve probe type.
Abdominal CT was performed on a 128 slice CT scanner.
Abdominal MRI examination was performed on a 1.5 Tesla MRI scanner.
Images acquisition done on multiple planes with T1-weighted (TR 631 ms; TE 9 ms) and T2-weighted Turbo Spin Echo (TR 5330 ms; TE 87 ms) sequences; fat-suppressed T2-weighted TSE images (TR 5838 ms; TE 87 ms).
Informed consent was obtained from either the parents or the patient herself.
Patient 1
A 16-years-old female presented with severe right lower abdominal pain accompanied with high fever.
There was also history of intermittent abdomino-pelvic pain since one year prior to admission which worsened a month before.
Gynecologic history revealed menarche at 13 years of age followed by irregular menses and dysmenorrhea.
Any recent abdominal trauma,
nausea,
vomiting,
diarrhea was denied.
Physical examination by rectal toucher indicated uterus deviated to the right,
also revealed palpable and tender pelvic mass,
sized approximately 8 x 8 cm with limited mobility.
Abdominal US was ordered and showed uterine cavities protruding to the right side and grossly distended,
filled with fluid suggesting hematometra.
Right kidney was absent (Fig.8).
Infected ovarian cyst was suspected at first and abdominal CT was performed prior to surgery.
Abdominal CT revealed uterus didelphys,
right adnexal complex cyst,
and left single kidney (Fig.
9-A-D).
Exploratory laparotomy was done and omentum covered cystic mass,
also enlarged uterus (suggesting uterus didelphys) were found (Fig.10). Then,
right salpingo-oophorectomy,
adhesiolysis,
and omentectomy were carried out.

Fig. 8: Abdominal USG findings of a 16-years-old female presented with severe right lower abdominal pain and high fever, turned out to be HWW syndrome, revealed uterine cavities protruding to the right side and grossly distended, filled with fluid,
suggesting hematometra. Right kidney was absent.
References: Department of Radiology, Dr. Soetomo General Hospital, Surabaya
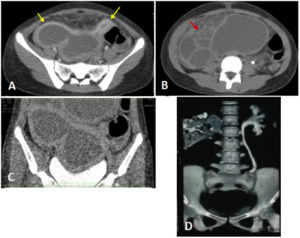
Fig. 9: Abdominal CT images of a 16-years-old female presented with severe right lower abdominal pain and high fever, turned out to be HWW syndrome. A) Axial and C) coronal CT image showed uterus didelphys (yellow arrow). B) Axial CT image showed right adnexal complex cyst (red arrow) D) 3D reconstruction showed left single kidney.
References: Department of Radiology, Dr. Soetomo General Hospital, Surabaya
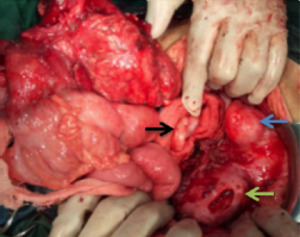
Fig. 10: Exploratory laparotomy of a 16-years-old female presented with severe right lower abdominal pain and high fever, turned out to be HWW syndrome, revealed omentum covered cystic mass (blue arrow), also enlarged uterus suggesting uterus didelphys (green arrow) were found. Left ovary seems normal (black arrow).
References: Department of Obstetrics and Gynecology, Dr. Soetomo General Hospital, Surabaya
Abdominal MRI performed afterwards revealed two separate uterine cavities and cervices suggestive of uterus didelphys with hematometrocolpos along right uterus cavity and cervical canal distension,
also right kidney agenesis (Fig.11).
Right hemivagina was dilated with blood products within,
implicating the presence of an obstructing right vaginal septum with a small communication exists between the duplicated cervices.
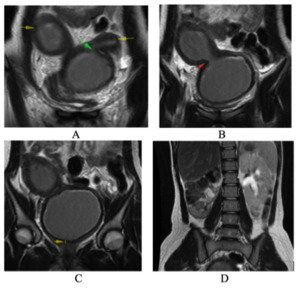
Fig. 11: Post surgery abdominal MRI images of a 16-years-old female presented with severe right lower abdominal pain and high fever, turned out to be HWW syndrome. A) Coronal T2 MRI showed uterus didelphys (yellow arrow) and incomplete obstructed hemivagina, there was communicating outflow between left uterine to the contralateral (green arrow); B) red arrow showed right cervical canal distension; C) right sided hematometrocolpos was demonstrated, indicating the presence of vaginal septum which observed as hypointense band ± 4 mm in thickness at mid vagina (yellow arrow); D) Coronal T2 MRI image showed absent right kidney.
References: Department of Radiology, Dr. Soetomo General Hospital, Surabaya
The patient was diagnosed with HWW syndrome and since there was communication between the duplicated cervices it falls into classification 2.2 according to the new HWW syndrome classification.
Transvaginal resection of the vaginal septum was done in order to drain the hematocolpos afterwards (Fig.12).

Fig. 12: Transvaginal resection of the septum to drain hematocolpos
References: Department of Obstetrics and Gynecology, Dr. Soetomo General Hospital, Surabaya
Patient 2
A 13-years-old female presented with left lower abdominal pain.
Gynecologic history revealed menarche at 12 years of age also followed by irregular menses and dysmenorrheal after then.
Palpable cystic mass,
sized approximately 5 x 8 cm at suprapubic with limited mobility was detected on physical examination.
Abdominal US then performed and showed uterus enlargement with hematometra and hematocolpos also a second uterus-like mass (Fig.13).
Abdominal MRI was performed for further evaluation and revealed uterus didelphys with left obstructive hemivagina (Fig.14A-C).
The abdominal MRI also revealed agenesis of left kidney (Fig.14D).
The findings were consistent with HWW syndrome (classification 1.1) and the patient also had transvaginal resection of the vaginal septum.
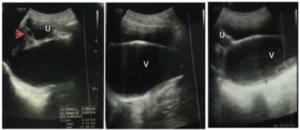
Fig. 13: Abdominal USG findings of a 13-years-old female presented with left lower abdominal pain, turned out to be HWW syndrome, showed uterus enlargement with fluid containing internal echoes suggesting hematometra (U) and hematocolpos (V) also a second uterus-like mass (red arrow).
References: Department of Radiology, Dr. Soetomo General Hospital, Surabaya
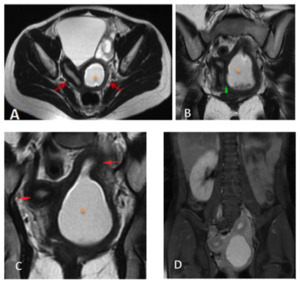
Fig. 14: Abdominal MRI images of a 13-years-old female presented with left lower abdominal pain, turned out to be HWW syndrome. A) Axial and C) Coronal T2 MRI image showed uterus didelphys (red arrow) with left obstructed hemivagina (orange star). B) Coronal T2 MRI image showed left obstructive hemivagina (orange star) indicating presence of vagina septum which observed as hypointense band, ± 2.7 mm in thickness (green head arrow), there is no communication between the duplication genital structure at any level C) Coronal T2 MRI image revealed left kidney agenesis.
References: Department of Radiology, Dr. Soetomo General Hospital, Surabaya
Patient 3
An 18-years-old female presented with lower abdominal and pelvic pain.
Those complaints occurred since the patient experienced menarche at 12 years of age.
There was also history of irregular menstruation and severe dysmenorrhea.
Upon physical examination there were fluid collection in vagina and palpable mass as well.
On abdominal US,
uterus enlargement and fluid collection in vagina,
consistent with hematometrocolpos were found.
Uterus didelphys with obstructed hemivagina was suspected.
Due to severe abdomino-pelvic pain,
immediate incision was performed to drain hematometrocolpos before any further imaging.
Abdominal MRI which was performed afterwards indicated uterus didelphys with two vaginas with vaginal septum ± 2.6 mm in thickness (Fig.15A-D).
The presence of right kidney agenesis (Fig.15-E),
made the patient diagnosed with HWW syndrome (classification 1.1).
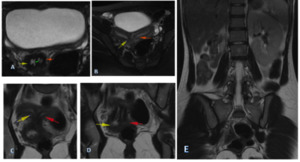
Fig. 15: Abdominal MRI images of an 18-years-old female presented with lower abdominal and pelvic pain which turned out to be HWW syndrome. A-D) Axial and coronal T2 MRI image showed two separate uterine with two separate cervices (uterus didelphys) (right: yellow arrow, left :red arrow) with vaginal septum ± 2.6 mm in thickness; E) Coronal T2 MRI image revealed right kidney agenesis.
References: Department of Radiology, Dr. Soetomo General Hospital, Surabaya
The demographic,
clinical characteristics and radiologic findings in all the 3 patients is summarized below (Fig.16 & Fig.17).
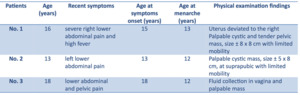
Fig. 16: Demographic and clinical characteristics of the 3 cases.
References: Department of Radiology, Dr. Soetomo General Hospital, Surabaya
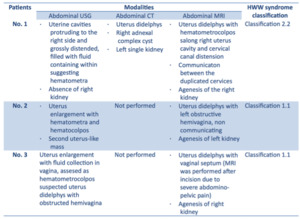
Fig. 17: Radiologic findings in 3 patients with HWW syndrome.
References: Department of Radiology, Dr. Soetomo General Hospital, Surabaya


 Axial and C) coronal CT image showed uterus didelphys (yellow arrow). B) Axial CT image showed right adnexal complex cyst (red arrow) D) 3D reconstruction showed left single kidney. References: Department of Radiology, Dr. Soetomo General Hospital, Surabaya")
, also enlarged uterus suggesting uterus didelphys (green arrow) were found. Left ovary seems normal (black arrow). References: Department of Obstetrics and Gynecology, Dr. Soetomo General Hospital, Surabaya")
 Coronal T2 MRI showed uterus didelphys (yellow arrow) and incomplete obstructed hemivagina, there was communicating outflow between left uterine to the contralateral (green arrow); B) red arrow showed right cervical canal distension; C) right sided hematometrocolpos was demonstrated, indicating the presence of vaginal septum which observed as hypointense band ± 4 mm in thickness at mid vagina (yellow arrow); D) Coronal T2 MRI image showed absent right kidney. References: Department of Radiology, Dr. Soetomo General Hospital, Surabaya")

 Axial and C) Coronal T2 MRI image showed uterus didelphys (red arrow) with left obstructed hemivagina (orange star). B) Coronal T2 MRI image showed left obstructive hemivagina (orange star) indicating presence of vagina septum which observed as hypointense band, ± 2.7 mm in thickness (green head arrow), there is no communication between the duplication genital structure at any level C) Coronal T2 MRI image revealed left kidney agenesis. References: Department of Radiology, Dr. Soetomo General Hospital, Surabaya")
 and hematocolpos (V) also a second uterus-like mass (red arrow). References: Department of Radiology, Dr. Soetomo General Hospital, Surabaya")
 Axial and coronal T2 MRI image showed two separate uterine with two separate cervices (uterus didelphys) (right: yellow arrow, left :red arrow) with vaginal septum ± 2.6 mm in thickness; E) Coronal T2 MRI image revealed right kidney agenesis. References: Department of Radiology, Dr. Soetomo General Hospital, Surabaya")

