ECR 2018 / C-1187
Systematic Approach to Pineal Region Lesions.
Congress:
ECR 2018
Poster Number:
C-1187
Type:
Educational Exhibit
Keywords:
Pathology, Education and training, Diagnostic procedure, MR, CT, Neuroradiology brain
Authors:
S. Moawad1, S. Hasan2, H. Semaan3, S. pinsky2, H. Elsamaloty3; 1Toledo, Ohio/US, 2Toledo/US, 3Toledo, OH/US
DOI:
10.1594/ecr2018/C-1187

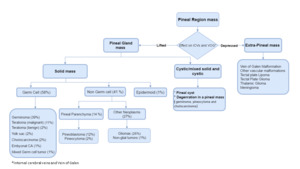
Fig. 2:
Algorithmic approach toward pineal region lesions

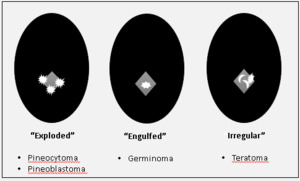
Fig. 3

Fig. 4:
Patterns of calcification

Fig. 5

Fig. 6

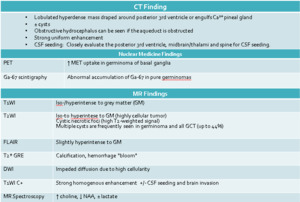
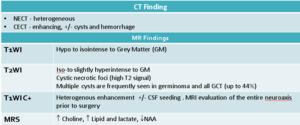
Fig. 7:
Imaging Characteristics of pineal germinoma

Fig. 8:
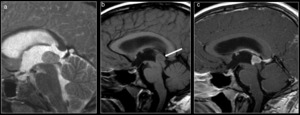
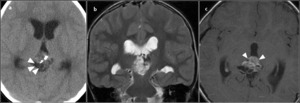
Axial NECT showing a lobulated homogenously hyperdense midline mass with...
 , T1WI (b) and T1WI+C (c) showing a T1 and T2 isointense germinoma with homogenous post contrast enhancement.")
Fig. 9:
Sagittal MRI T2WI (a) , T1WI (b) and T1WI+C (c) showing a T1 and T2 isointense...

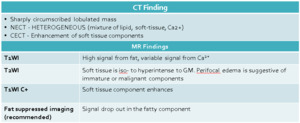
Fig. 10:
Imaging characteristics for pineal teratoma.
 showing a heterogenous pineal mass contain fat (arrowheads), soft tissue and calcifications.
Coronal T2WI (b) and axial T1WI+C (c) showing enhancing soft tissue component of the teratoma (arrowheads in c).")
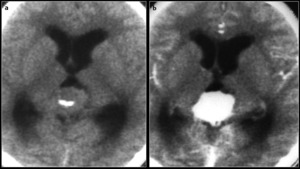
Fig. 11:
Axial CT image (a) showing a heterogenous pineal mass contain fat (arrowheads),...
 and CECT (b) showing a lobulated homogenously enhancing pineal gland mass with central calcifications. Note the hydrocephalus secondary to obstruction of the cerebral aqueduct. While imaging features are non specific, this was proven to be a yolk sac tumor following surgical excision.")
Fig. 12:
Axial NECT (a) and CECT (b) showing a lobulated homogenously enhancing pineal...
")
Fig. 13:
Table: Imaging Characteristics of pineal Choriocarcinoma.
Figure: Sagittal MRI...

Fig. 14:
Imaging Characteristics of pineal embryonal Carcinoma
 and T1WI + C (b) shows mixed solid-cystic pineal region mass with heterogenous enhancement. This was proven to be a mixed germ cell tumor after surgery.")
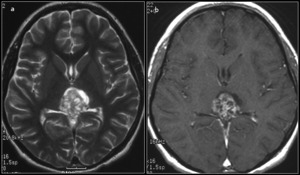
Fig. 15:
Axial T2WI (a) and T1WI + C (b) shows mixed solid-cystic pineal region mass...
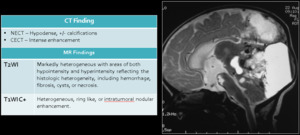
 Large heterogenous mass with “exploded”, peripheral calcification (arrowheads) with obstructive hydrocephalus (Image courtesy of James G. Smirniotopoulos, M.D)
B)Sagittal T1WI showing heterogenous pineoblastoma with areas of necrosis. Note the obstruction of the cerebral aqueduct (arrowhead), a common finding in pineoblastoma.")
Fig. 16:
Table: Imaging characteristics of Pineoblastoma
Figure: A) Large heterogenous...
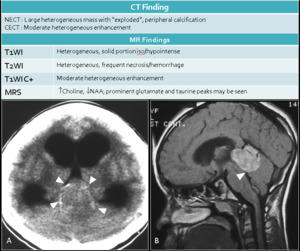
 showing homogenous enhancement of the pineocytoma. Axial T1WI (b) and axial T2WI (c) showing the pineoyctoma to be isointense to grey matter on T1 and hyperintense on T2.")
Fig. 17:
Table: Imaging characteristics of Pineocytoma.
Figure: Axial CECT (a) showing...
 indicating a retinoblastoma. The left eye has been enucleated for a retinoblastoma. There is an associated enhancing pineal PNET ( white arrow).")
Fig. 18:
Axial CECT images showing a trilateral retinoblastoma. Note the retinal...
, Axial T2WI (b) images showing a CSF signal intensity pineal cyst (arrow). Note the incomplete suppression on FLAIR (c).")
Fig. 19:
Table: Imaging characteristics of Pineal cyst
Figure: Sagittal T1WI (a), Axial...
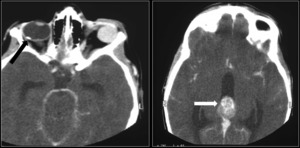
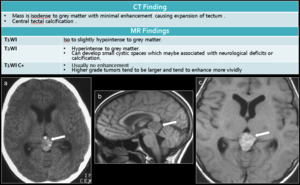
 showing tectal glioma with calcifications. Sagittal T1WI (b) show the mass to be hypointense to GM with enhancement on axial T1WI +C (c) The avid enhancement is atypical and suggests a high grade glioma.")
Fig. 20:
Table: Imaging Characteristics of tectal glioma.
Figure: Axial NECT (a)...
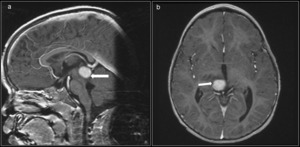
 and axial (b) T1WI +C showing avidly enhancing right thalamic pilocytic astrocytoma mimicking a pineal mass.")
Fig. 21:
Sagittal (a) and axial (b) T1WI +C showing avidly enhancing right thalamic...
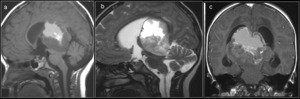
: Sagittal T1WI (a), sagittal T2wI and coronal T1WI +C show a heterogenous aggressive GBM resulting in obstructive hydrocephalus.")
Fig. 22:
Tectal Glioblastoma Multiforme (GBM): Sagittal T1WI (a), sagittal T2wI and...
Sagittal ultrasound Showing the vein of Galen malformation (VGAM) (arrows).
Brain MRI sagittal T1WC (B), T2W (C) and coronal T2W (D) demonstrating the VGAM (white arrows) and an associated hemorrhage (yellow arrow)")
Fig. 23:
A)Sagittal ultrasound Showing the vein of Galen malformation (VGAM)...
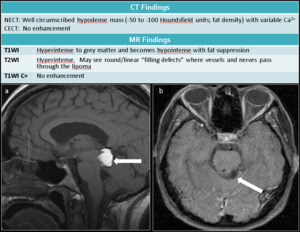
 shows well circumscribed hyperintense midline mass which demonstrates drop in signal on the axial T1-weighted fat saturated images (b) (arrow).")
Fig. 24:
Figure: Sagittal T1WI (a) shows well circumscribed hyperintense midline mass...