Technique of spinal ultrasound
•Spinal cord is easily analysable until 3rd month
• Through the posterior arches incompletely ossified.
• Infant in prone,
with pillow under the abdomen or lateral decubitus.
• Linear probe of high frequency (at least 7 MHz) with axial and longitudinal cuts from the occiput to the sacrum.
•Analysis of the bulbo-medullary junction: flexion of the neck oor phased-array that follows the physiological cervical lordosis of the infant.
Indications
- Clinical lumbosacral anomaly :
Cutaneous stigma at high risk of dysraphism:
- Angioma on the midline,
nevus.
- Subcutaneous mass.
- Tuft of hair or a pigmented spot.
- Caudal appendix.
- Aplasia or cutaneous hypoplasia.
- Dermal sinus.
- Sacred agenesis.
- High-risk coccygeal fossa: atypical fossa,> 5 mm in size and more than 2.5 cm from the anus.
Cutaneous stigma at high risk of dysraphism:
- Simple coccygeal fossa,
<5 mm and <2.5 cm from the anal margin.
- Or bony: hemi vertebrae,
dehiscence of the posterior arch.
2. Anorectal malformation
3.
Fight Bladder,
unexplained bladder globe ,
or repetitive urinary tract infections.
4.
Abnormal neurological examination of the lower limbs.
A normal spinal ultrasound eliminates severe dysraphism and provides an MRI.
Normal radio anatomy of spinal ultrasound :
1) The spinal cord:
- Marrow: hypoechoic tubular structure,
thicker in the cone region (about 5.5 mm)
thinner in the dorsal region (about 4.5 mm).
- Centered by a hyperechoic echo"complex central echo" : at the acoustic interface between the anterior white commissure and the central part of the anterior median fissure.
- Laterally,
the marrow is fixed by the serrated ligaments (arachnoidal duplications) which appear as fine linear echoes oriented transversely.
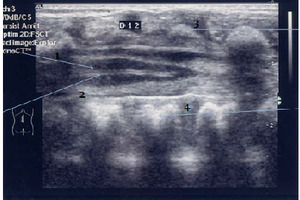
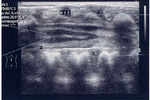
Fig. 1: 1 Spinal cord
2 Central canal of the spinal cord
3 Spinous process�
4 Body of vertebrae

Fig. 5: normal spinal cord
2) The cervico-occipital hinge
Sub-occipital sagittal section:
- Large cistern
- Cerebellar tonsils to eliminate a chiari malformation.
- Analyze the pons,
bulb and cervical spine
- Within the subarachnoid spaces
3) terminal conus medullaris :
- Conus medullaris : ends above L3.
Its terminal portion gradually tapered continues with the terminal filum whose thickness varies from 0.5 to 2 mm.
- Filum terminale visualized on the median line,
behind the roots.
Its thickness is = or less than 2 mm.
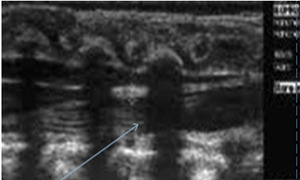
Fig. 2: filum terminale
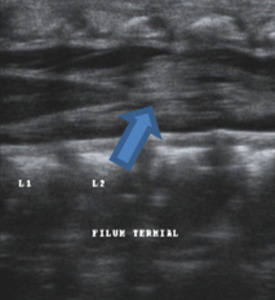
Fig. 4: filum terminale
•Lumbar and sacral roots (ponytail): echoic features,
arranged around and below the terminal cone.
•The ending of the space dural is in S2.
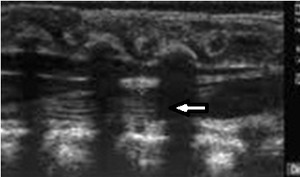
Fig. 3: Lumbar and sacral roots
Simple clinical and ultrasound landmarks to identify vertebral bodies,
and locate the terminal cone:
Clinical landmarks :
- The tip of the last rib is L2.
- The top of the iliac crest corresponds to L4.
Ultrasound landmarks :
- Follow the 12th coast until T12
- Visualization of the renal pedicle located at L2
- Possibly identifying the 1st sacral vertebra (in the absence of transitional anomaly).
The variants of the normal:
In about 10% of newborns.
1)The dilation of the terminal ventricle (rare):
- Anechoic formation,
- Ovoid v Clear limit
- Hyperechoic in the filum or in the conus medullaris
- Size <5mm
- Stability over time
2) Filum Terminale cyst:
- Origin discussed
- Arachnoid reflexion or embryonic remnant covered with ependymocytes.
- Less visible on MRI
- Strict criteria:
- Median line
- In the filum,
just below the spinal cone
- Fusiform
- Well limited
- Anechoic as a simple cyst.
3)Transient dilatation of terminal ependymal canal:
Differential diagnosis of syringomyelia and terminal ventricle.
4) Pseudo dermal sinus
- Fibrous tissue extended: cutaneous dimple → coccyx.
- Dermal sinus is rarely located at the tip of the coccyx and often more cranial.
- Search mass or liquid well along this fibrous tract.
5) Filum prominent
- More visible compared to nerve roots.
- Thickness> 1mm
- median
6) Coccyx:
•Many possible variations can be considered as a mass on palpation.